Hey thereif youre scrolling through endless pages trying to make sense of types of Rett syndrome, youve just landed in the right spot. In the next few minutes well cut through the jargon, walk through the main varieties, the four stages, what really causes this condition, and what life looks like for those living with it. No fluff, just the stuff youre actually looking for.
Quick Overview
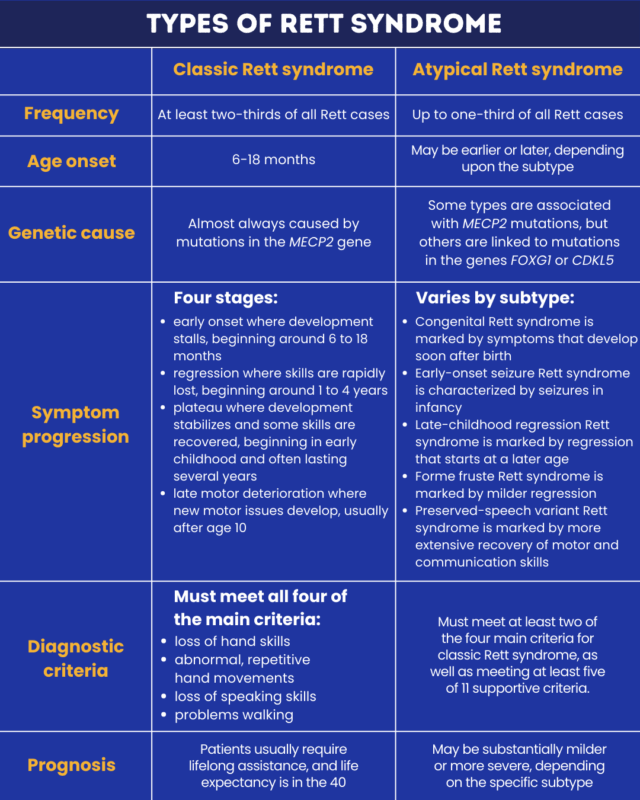
What are the main types of Rett syndrome?
Rett syndrome comes in two broad families: theclassic (or typical) form and theatypical (variant) forms. The classic type follows a wellcharacterised pattern of four stages, while the atypical variants bend those rulesdifferent genetic tweaks, slightly different symptoms, and sometimes a milder course.
Why does it matter?
Understanding which type youre dealing with shapes everything from treatment choices to longterm planning. It also gives families a clearer picture of prognosis, helps doctors target therapies, andlets be honestprovides a little peace of mind when the unknown feels overwhelming.
Classic Rett
What defines classic Rett syndrome?
The classic (or typical) form is what most textbooks describe when they talk about Rett. Its marked by a sudden loss of purposeful hand use, a characteristic handwringing motion, and a regression of spoken language. Youll also see gait disturbances and, as the child grows older, a range of behavioral and autonomic issues.
Which gene is behind it?
Over95% of classic cases are linked to mutations in the MECP2 gene on the X chromosome. This gene helps regulate other genes, so when its offbalance, a cascade of neurological changes follows.
Four stages of classic Rett
| Stage | Age Range | Main Features |
|---|---|---|
| Stage1 Early Onset | 618months | Subtle motor delays, slowed growth, loss of eye contact. |
| Stage2 Rapid Regression | 14years | Loss of speech, handwringing, motor skill decline, seizures may begin. |
| Stage3 Plateau | 210years | Improved motor control, but persistent gait issues and possible scoliosis. |
| Stage4 Late Motor Deterioration | Adolescenceadulthood | Reduced mobility, rigidity, increased risk of respiratory problems. |
A realworld glimpse
Take Maya, a bright toddler who began walking at 14months. At 2years she suddenly stopped using her hands to explore toysshe started wringing them instead. Her pediatrician ordered genetic testing, which confirmed a classic MECP2 mutation. Mayas story mirrors the classic progression, and early recognition helped her family access speechlanguage therapy and seizure management before the regression deepened.
Atypical Variants
Atypical Rett doesnt follow the textbook script, but its just as real. Researchers usually split it into three recognizable subtypes, each with its own quirks.
| Subtype | Core Features | Typical Gene(s) | Approx. Share |
|---|---|---|---|
| Preserved Speech Variant (Zappella) | Limited spoken language retained; milder motor issues. | MECP2 (milder mutations) | ~10% |
| Early Seizure Variant (Hanefeld) | Frequent early seizures, abnormal EEG, sometimes severe regression. | CDKL5, FOXG1 | ~5% |
| Perrytype / Severe Atypical | Profound motor impairment, limited eye contact, often no handwringing. | MECP2 (severe mutations) | <1% |
How do these subtypes differ from classic?
Think of classic Rett as a wellknown songsame melody, predictable verses. Atypical variants are like remixes: the core beat (MECP2 involvement) stays, but the tempo, instruments, and lyrics change. For example, kids with the Preserved Speech Variant often keep a few words, which can be a huge communication advantage. Meanwhile, the Early Seizure Variant may present with epilepsy before any handwringing appears, throwing doctors off balance if they only expect classic signs.
Diagnostic clues for each variant
- Zappella: Look for retained speech beyond age 2years and milder hand motor loss.
- Hanefeld: Earlyonset seizures (often before 6months) and abnormal EEG patterns.
- Perrytype: Very limited eye contact, severe motor delay, and often a more profound MECP2 mutation.
A parents voice
When we heard mama still echoing from my sons lips at age three, we felt a glimmer of hope that he wasnt lost in the typical regression, shares Elena, mother of a child with the Zappella variant. It reminded me that every Rett story is unique.
Causes & Genes
What causes Rett syndrome?
Rett syndrome is almost always caused by adenovo mutationmeaning the change appears for the first time in the child, not inherited from a parent. In the rare inherited cases, a mother may carry a mild MECP2 variant that slips past standard screening.
Which genes are involved?
Besides MECP2, clinicians also test for CDKL5 and FOXG1 when an atypical picture emerges. These genes have overlapping roles in brain development and synaptic function, which explains the shared symptoms across the spectrum.
Risk factors to know
Advanced maternal age and a family history of neurodevelopmental disorders slightly raise the odds, but because most mutations occur spontaneously, the overall risk remains low. Prenatal screening for MECP2 isnt routine yet, but you can discuss carrier testing with a genetic counselor if youre planning a family.
Expert insight
According to a recent , early genetic confirmation shortens the diagnostic odyssey by an average of 1.8years, allowing families to access targeted therapies sooner.
Diagnosis Tips
When should clinicians suspect Rett?
Redflag checklist:
- Loss of purposeful hand use after 6months.
- Handwringing or other repetitive hand movements.
- Regression of spoken language.
- Gait abnormalities (stifflegged walk, toewalking).
- Seizures, especially earlyonset.
How is the diagnosis confirmed?
First, a thorough clinical exam against the consensus diagnostic criteria. Then, a genetic test panelusually a blood samplechecks for MECP2, CDKL5, and FOXG1 mutations. Some centers also use wholeexome sequencing when the picture is unclear.
What about forme fruste presentations?
Forme fruste Rett is a mild, oftenoverlooked version where children display only a few hallmark signsperhaps subtle hand stereotypies without major language loss. Because the symptoms can be brushed off as just shyness, pediatricians sometimes miss it. Awareness of this milder phenotype is crucial for early intervention.
Life Expectancy
What is the typical life expectancy?
Modern medical care has dramatically improved outcomes. For classic Rett, median life expectancy now stretches into the early 40s to 50s. Atypical variants can vary: those with severe earlyonset seizures may have a shorter lifespan, while the Preserved Speech Variant often enjoys a longer, more independent life.
Factors that improve survival
- Multidisciplinary care teams (neurology, cardiology, pulmonology).
- Effective seizure control.
- Nutrition managementpreventing feeding difficulties and constipation.
- Respiratory support when needed (e.g., nighttime CPAP).
- Early physical and occupational therapy to maintain mobility.
A day in the life
Consider Alex, a 16yearold with the Zappella variant. He still says hello and please, attends a partially integrated high school, and enjoys weekly music therapy. Thanks to a coordinated care plan, his seizures are wellcontrolled, and his family reports a quality of life that feels, in Alexs words, pretty normal for me.
Facial Features
What facial features are commonly seen?
Rett syndrome often comes with a set of recognizable facial traits, sometimes called Rett face. Typical features include:
- Higharched palate.
- Sparse, often lightcolored hair.
- Bruxism (teeth grinding) especially during sleep.
- Frequent smiling with a slightly flat expression.
Where can you find reliable images?
Credible medical image libraries, such as the , provide retinaclear photos that can help families identify subtle signs without confusion.
Managing Care
What therapies are evidencebased?
Theres no cure yet, but a combination of interventions can make a huge difference:
- Physical & occupational therapy: Keeps joints flexible, improves hand function.
- Speech and augmentative communication: For kids who lose verbal ability, picture boards or speechgenerating devices sustain interaction.
- Seizure medication: Tailored to the individuals EEG pattern; newer agents have fewer sideeffects.
- Behavioral support: Addresses anxiety, sleep disturbances, and sensory sensitivities.
- Emerging research: Genetherapy trials targeting MECP2 are in early phases, offering cautious optimism.
Potential risks of interventions
Every treatment has tradeoffs. Some antiseizure drugs can cause fatigue or affect growth. Overaggressive physiotherapy might lead to joint strain if not carefully monitored. Thats why a balanced, individualized plancrafted with the input of a multidisciplinary teamis essential.
Balanced advice
We encourage families to stay informed, ask plenty of questions, and never feel pressured into onesizefitsall solutions. Your childs unique pattern of strengths and challenges deserves a plan that feels right for you.
Conclusion
Understanding thetypes of Rett syndromeclassic versus atypicalunlocks a clearer roadmap for care, advocacy, and hope. While classic Rett follows the welldocumented fourstage journey, the atypical variants remind us that every child writes their own story, often with subtle differences in genetics, symptoms, and outcomes. By staying alert to early signs, securing a precise genetic diagnosis, and embracing a balanced, multidisciplinary approach, families can improve quality of life and extend life expectancy.
Wed love to hear from you. What questions do you have about Rett syndrome? Have you or someone you know navigated the diagnostic maze? Share your experience in the comments, and lets keep the conversation goingbecause together, were stronger.
FAQs
What are the main differences between classic and atypical Rett syndrome?
Classic Rett follows four predictable stages with hand‑wringing, loss of purposeful hand use, and regression of language. Atypical variants present varied patterns—some retain speech, others have early‑onset seizures, or display different motor behaviours—and are often linked to mutations in genes such as CDKL5 or FOXG1.
At what age does the regression phase usually begin in classic Rett?
The rapid regression (Stage 2) typically starts between 12 and 30 months, when children suddenly lose purposeful hand use, spoken words, and may develop the characteristic hand‑wringing movements.
Which genes are tested when a doctor suspects an atypical form of Rett syndrome?
In addition to MECP2, clinicians evaluate CDKL5 and FOXG1, because mutations in these genes can produce Rett‑like features, especially early‑onset seizures or milder speech preservation.
How can families improve life expectancy for someone with Rett syndrome?
Coordinated multidisciplinary care—regular seizure monitoring, respiratory support, nutrition management, physiotherapy, and early communication therapies—has lifted median survival into the 40s–50s for classic Rett and can similarly benefit atypical forms.
Is there any curative treatment for Rett syndrome currently available?
No cure exists yet, but ongoing gene‑therapy trials targeting MECP2 show promise. Meanwhile, symptom‑focused treatments and supportive therapies can markedly enhance quality of life.