Quick Start Overview
When is a CT ordered? Almost every suspected acute stroke gets a noncontrast CT within minutes of arrival. Its fast, widely available, and the best tool to rule out a hemorrhage before giving clotbusting drugs.
What does the scan aim to do? The primary goals are to (1) detect any intracerebral bleed, (2) spot early signs of ischemia, and (3) give a quick anatomical map for treatment decisions.
| Feature | CT | MRI |
|---|---|---|
| Speed | Minutes (often <5) | Usually 1030min, may need scheduling |
| Bleed detection | Excellent (hyperdense blood) | Good, but can miss subtle bleed early |
| Early ischemia | Subtle, requires expertise | Diffusionweighted imaging shows changes within minutes |
| Availability | Every hospital | Limited to centers with MRI suites |
Having this quick comparison in mind helps you understand why CT remains the gold standard in the hyperacute window.
Acute Ischemic Findings
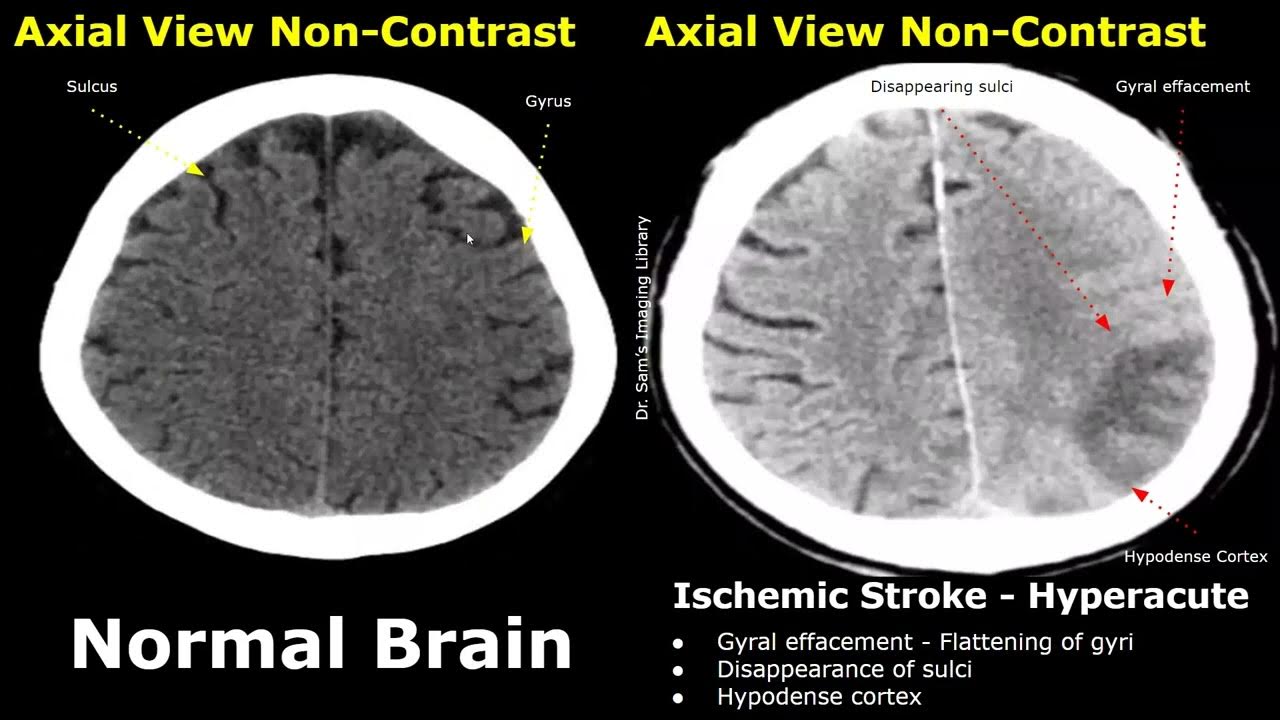
Ischemic strokes are caused by a blockage that cuts off blood flow. On a CT, the changes can be very subtle in the first few hours, but there are a few telltale clues you can learn to spot.
What are the classic early CT signs?
- Hyperdense artery sign a bright, dense appearance of a major artery (often the middle cerebral artery) indicating a clot inside.
- Loss of graywhite differentiation the boundary between the gray cortex and underlying white matter looks fuzzy.
- Insular ribbon sign the normally crisp insular cortex becomes obscured.
When do these signs become visible?
In the first 06hours, the hyperdense artery sign may be the only clue. Between 612hours, loss of graywhite differentiation becomes more noticeable. After 12hours, youll start seeing hypodensity (dark areas) as the tissue begins to infarct.
Why does it matter?
Identifying these early signs can tip the scales toward giving intravenous alteplase (tPA), which dramatically improves outcomes if administered within the therapeutic window.
Hemorrhagic Findings
If the CT shows bright, dense blood, youre looking at a hemorrhagic stroke. The appearance varies with the type of bleed.
Typical appearance of an intracerebral hemorrhage
It shows up as a hyperdense (bright) region in the brain parenchyma, often with surrounding hypodense edema that swells as the blood irritates nearby tissue.
Subarachnoid or subdural bleed?
Subarachnoid hemorrhage spreads thinly over the brains surface, looking like bright curvilinear lines in the sulci. Subdural bleeds sit between the dura and arachnoid layers, often crescentshaped and may cross suture lines.
Quick reference table
| Finding | Ischemic Stroke | Hemorrhagic Stroke |
|---|---|---|
| Density | Initially normal or slightly hypodense | Hyperdense (bright) |
| Shape | Diffuse or focal loss of graywhite border | Round, lobar, or crescentshaped collection |
| Location | Vascular territories | Often deep (basal ganglia) or lobar |
These distinctions are lifesaving because giving clotbusting medication to someone with a bleed can be catastrophic.
Acute vs Chronic Infarct
Sometimes a CT will show an area that looks old versus new. Knowing the difference prevents unnecessary alarm.
How does density change over time?
Acute infarcts are often isodense or slightly hypodense, sometimes with subtle swelling. After a few weeks, they evolve into welldefined, lowdensity (dark) cavities called encephalomalacia, often accompanied by enlarged ventricles or sulci.
What does gliosis look like?
In chronic lesions, you may see a thin rim of slightly higher density from scar tissue (gliosis). This rim is absent in fresh strokes.
Stepbystep decision tree
- Check density: bright = bleed, dark = chronic infarct, same as brain = possibly acute.
- Look for surrounding edema: prominent in acute, minimal in chronic.
- Assess ventricle size: enlarged ventricles suggest old volume loss.
When available, comparing the current study to prior imaging is invaluable; if prior scans show the same finding, it strongly suggests a chronic change rather than an acute event. For patients with complex neurologic histories (for example, those being evaluated for conditions like atypical Rett syndrome), this comparison can clarify whether an imaging abnormality reflects chronic developmental changes or a new vascular process.
CT vs MRI
Both modalities have a role, but they shine at different moments.
When is CT still king?
When seconds count. In the emergency setting, CT can be performed while the patient is on the stretcher, revealing a bleed in under five minutes.
When does MRI take over?
If the CT is negative but symptoms persist, MRIespecially diffusionweighted imaging (DWI)detects tiny ischemic lesions that CT might miss. MRI also provides better detail on the brainstem, posterior fossa, and early microinfarcts.
Sidebyside infographic idea
Imagine a split screen: left side shows a bright, welldefined bleed on CT; right side shows a faint DWI hyperintensity that confirms an early ischemic stroke. This visual helps clinicians decide when to order the next test.
Reading Checklist
Want a quick cheatsheet you can print and stick by your workstation? Heres a simple ABCD checklist tailored for stroke CT interpretation.
A Airway & Artifacts
Make sure the scan is free of motion artifacts. Bad images can hide key signs.
B Bleed?
Look first for hyperdense blood. If you see any, note the location, size, and surrounding edema.
C Clockface Distribution
Assess whether the abnormality follows a vascular territory (e.g., MCA distribution). This helps differentiate true stroke from mimics.
D Diffusionlike Signs (CT analogues)
Search for hyperdense artery, loss of graywhite differentiation, or subtle hypodensity hinting at early infarction.
Printable Table
| Finding | Interpretation | Action |
|---|---|---|
| Hyperdense artery | Clot in vessel | Consider tPA if within window |
| Bright intracerebral bleed | Hemorrhagic stroke | Hold anticoagulants, neurosurg consult |
| Old lacunar cavity | Chronic infarct | No acute action needed |
Common Pitfalls
Even seasoned radiologists can trip up. Here are the most frequent mistakes and how to avoid them.
Normal agerelated changes mistaken for early infarct
Small periventricular lowdensity spots are common in older adults. Crosscheck with the patients history and look for accompanying edema before calling it acute.
Posterior fossa artifacts masquerading as bleed
Bone can cause bright streaks that look like blood. Adjust the window level, or scroll through multiple slices to confirm.
Miniquiz (try before reading answers)
- Slice shows a bright crescent in the right hemisphere, crossing sutures. What is it?
- A subtle loss of graywhite border in the left insula, no bleed. What does it suggest?
- Large, welldefined lowdensity area with enlarged ventricle. Old or new?
Answers: 1) Subdural hemorrhage. 2) Early ischemic change. 3) Chronic infarct.
Case Studies
Stories stick better than bullet points. Below are four realworld snapshots that illustrate the spectrum of stroke CT interpretation.
CaseA: Hyperdense MCA Sign
A 55yearold man arrived with sudden righthand weakness. His CT showed a bright, dense middle cerebral arterya classic hyperdense artery sign. The team administered tPA within 2hours, and the patient regained full motor function. Key takeaway: Spotting that bright artery can be the difference between recovery and permanent deficit.
CaseB: Missed Early Ischemia
A 71yearold woman presented with slurred speech. The initial CT looked normal to the oncall radiologist, but a subtle loss of graywhite differentiation was present on a second review. Because tPA was delayed, she suffered a larger infarct. Lesson: Even tiny changes matterdoublechecking is worth the few extra minutes.
CaseC: Large Intracerebral Hemorrhage
A 62yearold man collapsed with a severe headache. CT revealed a massive hyperdense bleed in the basal ganglia, compressing the ventricle. Immediate neurosurgical evacuation was performed, saving his life. Takeaway: Rapid identification of bleed is critical to prevent fatal intracranial pressure spikes.
CaseD: Chronic Lacunar Mistaken for New Bleed
A 68yearold patients followup CT showed a small lowdensity spot in the thalamus. The attending thought it might be a new bleed and ordered unnecessary labs. Review of prior imaging confirmed it was a chronic lacunar infarct. Lesson: Always compare with old scans when possible.
Resources & Next Steps
Staying sharp means keeping up with guidelines and practice tools.
Guidelines
The American Heart Association/American Stroke Associations 2024 Imaging in Acute Stroke guideline offers the latest recommendations on when to use CT versus MRI.
Learning Platforms
For handson practice, check out the its packed with annotated cases that let you test your interpretation skills. Another great resource is the free online modules from the Radiology Masterclass, which walk through each CT sign step by step.
Stay Updated
Join our monthly Stroke Imaging Slack community where clinicians share challenging cases, new research, and quick tips. Its a supportive space that keeps your knowledge fresh without feeling like a lecture.
Conclusion
Understanding stroke CT scan interpretation isnt just a boxchecking exerciseits a lifesaving skill. By learning to spot the hyperdense artery sign, differentiate bleed from infarct, recognize chronic scars, and use a systematic checklist, you empower yourself (or your team) to make faster, smarter decisions. Keep practicing with real cases, lean on trusted guidelines, and dont hesitate to ask a colleague when something feels off. Every scan you read brings you one step closer to better outcomes for the patients who need it most.
FAQs
What is the primary purpose of a noncontrast CT scan in acute stroke?
It is mainly to quickly detect intracerebral hemorrhage, identify early ischemic signs, and provide an anatomical overview critical for treatment decisions.
What are classic early CT signs of acute ischemic stroke?
Key signs include the hyperdense artery sign indicating a clot, loss of gray-white matter differentiation, and the insular ribbon sign.
How can hemorrhagic stroke be distinguished from ischemic stroke on CT?
Hemorrhagic stroke appears as hyperdense (bright) blood collections, often round or crescent-shaped, while ischemic stroke initially shows subtle hypodensity or loss of normal brain differentiation.
Why is differentiating acute from chronic infarcts important on CT?
Because chronic infarcts show well-defined low-density areas often with gliosis and enlarged ventricles, while acute infarcts may have subtle swelling and less-defined hypodensity; this avoids unnecessary treatments.
When should MRI be preferred over CT in stroke imaging?
MRI, especially diffusion-weighted imaging, is preferred when CT is negative but symptoms persist, as it detects early ischemic changes and small infarcts more sensitively.