If youve just heard the word hysterectomy and feel a knot in your stomach, youre not alone. The first thing to clear up is which kind of surgery is right for you, because the three main typestotal, supracervical (partial) and radicaleach remove different parts of the reproductive tract and have distinct recovery paths.
Below youll get a quick rundown of each type, how doctors decide which is best for fibroids or other conditions, what recovery looks like, and a few gentle tips for you (and your partner) to stay comfortable after the operation.
Why It Matters
Understanding the differences isnt just academic; its about balancing benefits with risks, and feeling confident when you sit down with your surgeon. When you know what each approach entails, you can ask the right questions, set realistic expectations, and avoid unnecessary anxiety.
Three Core Categories
What Are the Three Main Types?
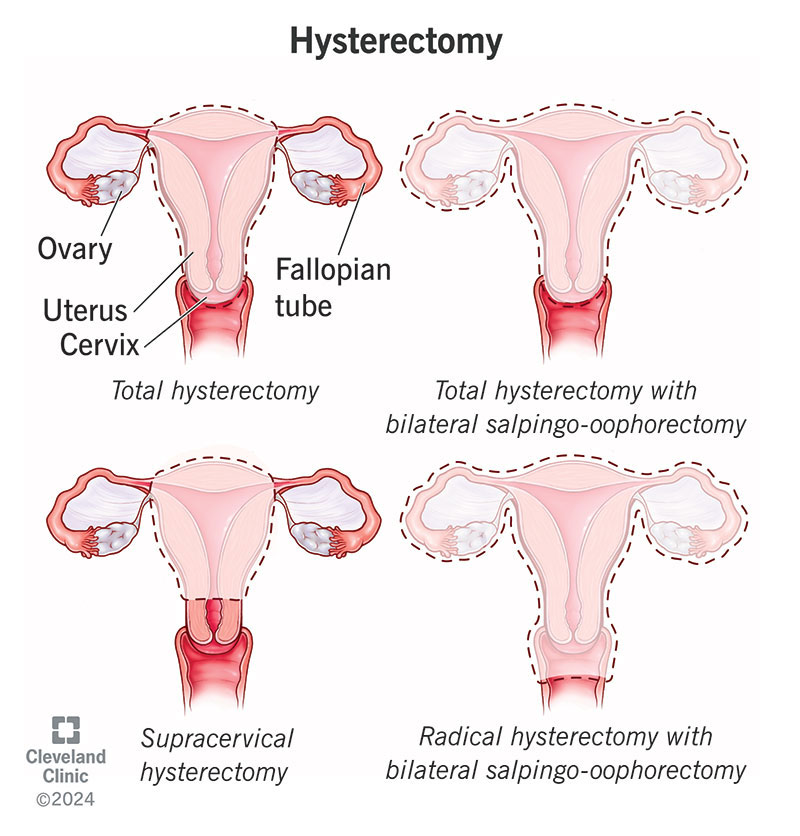
Total hysterectomy removes the uterus+cervix (the ovaries may stay). Supracervical (partial) hysterectomy removes only the uterus, leaving the cervix intact. Radical hysterectomy goes further, taking the uterus, cervix, and surrounding tissueusually reserved for cancer cases.
Quick Comparison
| Type | Whats Removed | Typical Indications | Recovery Time |
|---|---|---|---|
| Total | Uterus + cervix (ovaries optional) | Large fibroids, severe bleeding, cancer risk | 46 weeks |
| Supracervical | Uterus only | Benign disease, desire to keep cervix | 35 weeks |
| Radical | Uterus, cervix, parametrial tissue | Cervical or uterine cancer | 68 weeks+ |
How 5 Types of Hysterectomy Fit In
When you hear 5 types of hysterectomy, people are usually mixing the anatomical categories above with the surgical approaches: abdominal, vaginal, laparoscopic, roboticassisted, and handassisted. Think of the anatomy (whats removed) as the what, and the approach (how the surgeon gets there) as the how. Both choices shape your experience.
Total Hysterectomy
When Is It the Best Choice for Fibroids?
If youve got huge, multiple fibroids that keep growing despite medication, a total hysterectomy often offers the cleanest solution. According to the , removing both uterus and cervix eliminates the source of bleeding and pain, and it reduces the risk of future fibroid recurrence.
Expert Tip
Most OBGYNs will order a pelvic MRI or a detailed ultrasound before recommending a total hysterectomy. Those images let the surgeon see the exact size, location, and number of fibroids, which helps decide whether a less extensive surgery could work.
Pros and Cons
- Pros: Complete removal of the disease source, no need for future uterine surveillance, eliminates cervical cancer risk.
- Cons: If ovaries are removed, you may experience surgical menopause, which brings hot flashes, mood swings, and bone density changes.
Supracervical (Partial) Hysterectomy
Why Some Women Keep Their Cervix
Leaving the cervix behind can feel more natural for many. Some women say they experience a stronger sense of pelvic floor support, and they avoid the rare but possible condition called vaginal cuff dehiscence (a tiny tear where the cervix used to be).
RealWorld Anecdote
Emily, a 38yearold teacher, wrote in her recovery journal: I was nervous about keeping my cervix, but three months later I still feel steady when I jog. The scar healed quickly, and I didnt have any weird discharge. Stories like Emilys add a human layer to the data.
Recovery Nuances
Because the cervix stays, the surgical site is slightly smaller than a total hysterectomy, often translating to a shorter hospital staysometimes just one night. However, a small percentage of women develop cervical stump problems, like bleeding or pain, so followup appointments are essential.
Radical Hysterectomy
When Cancer Calls for Aggressiveness
Radical hysterectomy is reserved for earlystage cervical or uterine cancers that havent spread far. Its a lifesaving procedure, but it also carries the highest risk profile among the three core types.
Data Point
Recent National Comprehensive Cancer Network (NCCN) guidelines show a 5year survival rate of about 7080% for earlystage cervical cancer when a radical hysterectomy is performed, underscoring its effectiveness when truly needed.
Risks and Recovery
- Longer operative time and larger incision (often abdominal).
- Higher likelihood of urinary and bowel dysfunction after surgery.
- Recovery may stretch to 8weeks or more, with pelvic physical therapy often recommended.
Minimally Invasive Approaches
Laparoscopic & Robotic Types
When surgeons talk about laparoscopic hysterectomy types, theyre usually referring to three flavors: standard laparoscopy (small cameras and instruments), handassisted laparoscopy (a small hand port for extra control), and roboticassisted laparoscopy (the Da Vinci system). All aim to shrink the incision size, reduce blood loss, and speed up your return to daily life.
Video Suggestion
For a clear visual of what happens during a laparoscopic hysterectomy, you can watch a reputable from Cleveland Clinic. Seeing the procedure in action can demystify the process and ease anxiety.
Benefits of Going Small
- Incisions usually under 1cmso youll have fewer visible scars.
- Most patients walk out of the hospital the same day or next morning.
- Return to light activities in 23 weeks, full activity by 68 weeks.
Vaginal and Abdominal Routes
When Surgeons Pick One Over the Other
A vaginal hysterectomy means the uterus is removed through the birth canalno belly incision at all. Its ideal when the uterus isnt overly enlarged and theres enough vaginal space. An abdominal hysterectomy, on the other hand, involves a larger bellybutton incision, often used for very large fibroids or when the surgeon needs a broader view.
Checklist: Signs You Might Need a Hysterectomy
- Heavy, prolonged menstrual bleeding that doesnt respond to medication.
- Pelvic pain that interferes with work or sleep.
- Large fibroids compressing nearby organs.
- Endometrial cancer or severe precancerous changes.
Choosing the Right Type for Your Condition
What Type Is Best for Fibroids?
The consensus from the American College of Obstetricians and Gynecologists (ACOG) is that the choice hinges on fibroid size, location, and your personal goals. Small, welllocated fibroids might be managed with a laparoscopic myomectomy (fibroid removal) instead of a full hysterectomy. For massive, multiple fibroids, a total laparoscopic or robotic hysterectomy often offers the quickest relief. If youre also dealing with persistent pelvic pain and want to explore causes such as endometriosis, reading about pelvic pain endometriosis can help you understand whether hysterectomy would address the root issue or if other treatments should be tried first.
Questions to Ask Your Surgeon
- Will my ovaries be removed, and why?
- Which surgical approach do you recommend and why?
- Whats the expected length of hospital stay?
- How soon can I resume work, exercise, and sexual activity?
- What pain control options will be available?
- Are there any longterm hormonal considerations?
- How will my recovery be monitored after discharge?
Recovery & Pain Management
Typical Timeline After Each Surgery
Heres a sample 7day schedule for a laparoscopic hysterectomyfeel free to adapt it if youve had a different approach.
| Day | Activity | Notes |
|---|---|---|
| 1 | Hospital recovery | Light walking every 2hours; pain meds as prescribed. |
| 23 | Home rest | Short walks around the house; avoid heavy lifting. |
| 45 | Gentle stretching | Pelvic floor exercises (Kegels) if approved. |
| 67 | Light chores | Gradually increase activity; monitor incision sites. |
Pain Control Options
Most surgeons start with scheduled nonopioid analgesics (acetaminophen + ibuprofen) and add a short course of opioids only if needed. Some centers also offer a transverse abdominis plane (TAP) blockessentially a numbthearea injection that can reduce opioid use.
Lifestyle Tips for a Smoother Heal
- Nutrition: Proteinrich foods, plenty of water, and VitaminC to help tissue repair.
- Pelvic floor physio: A certified therapist can guide you through gentle exercises that restore strength and prevent urinary issues.
- Sleep hygiene: Keep your head slightly elevated to reduce swelling, and aim for 79hours of restful sleep.
Advice for Husbands (or Partners) After Hysterectomy
Supporting someone after surgery isnt just about cooking mealsits also emotional. Encourage your loved one to talk about fears, help with grocery runs, and be patient with mood swings that can stem from hormonal shifts or postoperative pain. A simple Im here for you can go a long way.
Putting It All Together
Choosing the right type of hysterectomy surgery is a deeply personal decision, shaped by medical facts, lifestyle goals, and emotional readiness. By understanding the three core categories (total, supracervical, radical) and how they intersect with surgical approaches (laparoscopic, robotic, vaginal, abdominal), you empower yourself to have an informed conversation with your doctor.
Remember, theres no onesizefitsall answer. Some women thrive after a minimally invasive total hysterectomy, while others find comfort in keeping their cervix with a supracervical procedure. The key is to weigh the pros and cons, ask the right questions, and lean on a supportive networkincluding that special someone whos willing to bring you soup and a listening ear.
Conclusion
In a nutshell, the types of hysterectomy surgery landscape is richer than a simple definition its a blend of anatomy, technique, and personal values. Whether youre wrestling with heavy bleeding, stubborn fibroids, or a cancer diagnosis, knowing the options helps you steer the conversation toward the safest, most effective path for you. If youre ready to take the next step, consider downloading a printable decisionmaking checklist (available on many clinic websites) or setting up a followup appointment to discuss any lingering questions. You deserve clear, compassionate careand a clear road to feeling like yourself again.
FAQs
What are the main types of hysterectomy surgery?
The three core types are total hysterectomy (removal of uterus and cervix), supracervical or partial hysterectomy (removes uterus but leaves cervix), and radical hysterectomy (removes uterus, cervix, and surrounding tissues, usually for cancer).
How is the type of hysterectomy chosen for fibroids?
Surgeons consider fibroid size, number, location, and patient goals. Total hysterectomy is common for large or multiple fibroids, while smaller fibroids might be managed laparoscopically or with myomectomy.
What are the surgical approaches for hysterectomy?
The approaches include abdominal, vaginal, laparoscopic, robotic-assisted, and hand-assisted surgeries. These determine how the surgeon accesses the uterus and affect recovery times.
What is the typical recovery time after a hysterectomy?
Recovery varies by type: total hysterectomy usually needs 4–6 weeks; supracervical about 3–5 weeks; radical can be 6–8 weeks or more. Minimally invasive techniques often reduce recovery duration.
Are there any risks specific to radical hysterectomy?
Yes, radical hysterectomy carries higher risk of urinary and bowel dysfunction and longer hospitalization due to removal of additional tissues and more extensive surgery.