If your eyepressure numbers look normal but your doctor still says you have glaucoma, youre probably wondering whether any treatment is even necessary. The short answer is yes keeping the pressure from spiking and protecting the optic nerve can still make a huge difference in preserving your vision.
In the next few minutes Ill walk you through the most reliable, evidencebacked options for managing this sneaky form of the disease, lay out the pros and cons of each, and give you practical tips you can bring straight to your next eyedoctor visit. Think of it as a friendly cheatsheet you can actually use.
Why Treat NTG?
What is normaltension glaucoma?
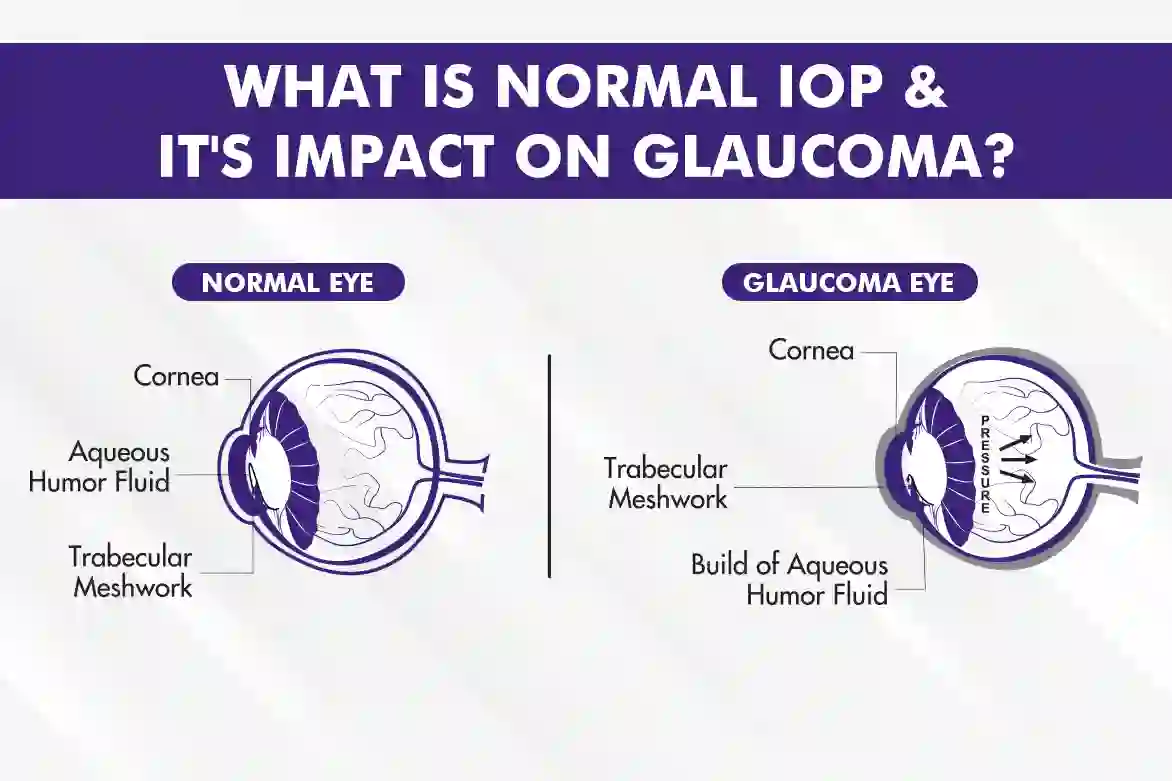
Normaltension glaucoma (NTG), sometimes called lowpressure glaucoma, is a type of opticnerve damage that occurs even though the intraocular pressure (IOP) stays within the normal range of 1021mmHg. About onethird of all glaucoma cases worldwide fall into this category, and it tends to show up more often in people of Asian descent and in those with a family history of the disease.
How can normal pressure still damage the optic nerve?
Even when the numbers look fine, the optic nerve can be vulnerable for several reasons. Fluctuations in pressure throughout the day, reduced blood flow to the retina, or a thinner, weaker connective tissue sheath around the nerve can all make the nerve more susceptible to damage. Think of it like a garden hose thats not under high pressure but still has a kink the flow (or in this case, oxygen) is compromised.
Is normaltension glaucoma hereditary?
Theres a genetic component, but its not a simple you get it from Mom situation. Studies show that having a firstdegree relative with NTG raises your risk by about 23times, yet lifestyle and vascular health play major roles too. So while you cant change your DNA, you can influence the other factors that decide how quickly the disease progresses.
Medical FirstLine Options
Prostaglandin analogs
These eye drops are the workhorse for most glaucoma patients because they increase fluid outflow from the eye, typically lowering IOP by 2530%. Even though the baseline pressure is normal, a modest drop can still slow the loss of visual field. Common brands include latanoprost (Xalatan) and travoprost (Travatan). Side effects are usually mild a bit of eyelash growth or darkening of the iris, which many people find acceptable.
Alpha2 agonists and other drops
If a prostaglandin alone isnt enough, doctors often add an alpha2 agonist such as brimonidine or a carbonic anhydrase inhibitor like dorzolamide. These medications work by either reducing fluid production or further enhancing outflow. Combination therapy can achieve an extra 510% pressure reduction, which research shows can meaningfully delay visualfield loss.
Oral carbonic anhydrase inhibitors
For tougher cases where drops dont do the trick, oral agents like acetazolamide may be prescribed. Theyre powerful at lowering pressure but can cause systemic side effects tingling in the fingers, mild fatigue, and occasional kidney stones. Because of these risks, theyre usually reserved for shortterm bridge therapy while other treatments take effect.
Comparison of Medications
| Medication Type | Typical IOP Reduction | How Often Used | Common Side Effects |
|---|---|---|---|
| Prostaglandin analog | 2530% | Once daily | Eyelash growth, iris darkening |
| Alpha2 agonist | 1520% | 23 times daily | Dry mouth, mild fatigue |
| Topical carbonic anhydrase inhibitor | 1520% | 23 times daily | Burning sensation, bitter taste |
| Oral carbonic anhydrase inhibitor | 2025% | Shortterm | Tingling, nausea, kidney stones |
These numbers come from a metaanalysis published in the , which pooled data from more than a dozen clinical trials.
Laser Treatment Options
Selective laser trabecular microsurgery (SLT)
SLT uses a brief, lowenergy pulse to target pigmented cells in the trabecular meshwork, improving fluid outflow without causing scar tissue. Its an attractive option when drops arent enough, because it can lower pressure by about 1520% and the effect often lasts 24years. Plus, theres no incision and recovery is essentially immediate.
Argon laser trabeculoplasty (ALT)
ALT is an older technique that applies a longerduration laser to the same area. Its still used in some clinics, especially where SLT isnt available, but it carries a slightly higher risk of inflammation and may cause more permanent changes to the eyes drainage system.
Cyclodiode laser for advanced cases
When the disease has progressed despite meds and conventional laser, cyclodiode laser can be employed to reduce the eyes production of fluid. Its considered a lastditch lowpressure glaucoma treatment because it can also affect surrounding tissue, so careful patient selection is crucial.
Patient Story
Mark, a 58yearold accountant from Denver, was diagnosed with NTG after noticing subtle peripheral vision loss during a routine eye exam. He tried prostaglandin drops for a year, but his visual field kept shrinking. After a single SLT session, his doctor said the pressure drop was enough to break the progression curve. Six months later, Marks latest test showed a stable field, and hes now able to drive at night without anxiety.
Surgical Intervention Paths
Trabeculectomy
Trabeculectomy creates a tiny drainage flap under the conjunctiva, allowing fluid to bypass the normal outflow pathways. Its the goldstandard surgery for glaucoma and can lower IOP by 3050% even when the starting pressure looks normal. The downside? A small risk of infection (blebitis) and the need for postoperative eyedrops to keep the flap functional.
Tubeshunt implants
When the eyes own drainage zone is scarred or compromised, a small tube (often made of silicone) can be implanted to channel fluid to a reservoir plate under the eyelid. Tube shunts are favored for eyes that have failed previous surgeries. Theyre very effective, but they can cause a mild, chronic bubbly feeling in the eye and, rarely, tube erosion.
MIGS microinvasive glaucoma surgery
Microinvasive procedures such as the iStent or Hydrus Microstent are designed to be less aggressive than traditional surgery. They are often performed together with cataract surgery. While MIGS can drop pressure by about 1015%, many specialists are still debating whether theyre powerful enough for NTG, where every millimeter counts. If you also have cataract concerns, discussing cataract options and whether cataract surgery could be combined with a microstent may be useful learn more about cataract diagnosis and how it can affect surgical planning by reviewing a cataract diagnosis test.
DecisionMaking Flowchart
Imagine a simple flowchart:
- Start with drops adequate control? Yes: stay on meds.
- If not, try SLT adequate control? Yes: monitor.
- If still progressing, consider trabeculectomy adequate control? Yes: continue followup.
- If surgery not tolerated, evaluate tubeshunt or MIGS based on eye anatomy and lifestyle.
This stepwise approach helps keep treatment as minimally invasive as possible while still protecting vision.
Adjunct Lifestyle Strategies
Optimizing ocular blood flow
Because NTG often involves inadequate blood supply to the optic nerve, cardiovascular health matters. Regular aerobic exercise (like brisk walking for 30minutes most days) can improve circulation, while avoiding extreme activities that spike blood pressure. Some patients also benefit from omega3rich foods think salmon, walnuts, and flaxseed.
Managing systemic risk factors
Conditions such as sleep apnea, hypertension, and migraines have been linked to faster NTG progression. If you have any of these, work with your primary care doctor to keep them under control. Even simple steps like sleeping on your side (instead of flat on your back) can reduce nocturnal eyepressure spikes.
Monitoring disease progression
Regular visualfield testing, usually every 612months, is essential. The first sign of glaucoma is often a subtle loss of peripheral vision, which most people dont notice in everyday life. Thats why scheduled tests are your best defense they catch changes before youre even aware of them.
FAQ Snapshot
Will I go blind from normaltension glaucoma? The risk is low if the disease is caught early and treated consistently. Most patients retain functional vision for decades.
How fast does normaltension glaucoma progress? It varies widely; some people stay stable for years, while others experience faster field loss if vascular risk factors are present.
What are common symptoms? Peripheral vision loss, difficulty seeing in low light, and occasional shadow or glare sensations.
Risks & Benefits
Benefits of lowering IOP even when normal
Research shows that even a modest 10% reduction can significantly slow visualfield loss in NTG. Its like turning down the volume on a leaky faucet the slower the flow, the longer your optic nerve lasts.
Potential side effects
Each treatment carries its own risk profile. Drops can cause eye irritation or systemic symptoms; laser may cause temporary inflammation; surgery carries infection and scarring risks. Being aware of these helps you weigh the options with your doctor.
Balancing options with personal goals
Some people prefer a medicationonly approach because its noninvasive, while others are ready to jump to laser or surgery for a more permanent solution. Think about your lifestyle, tolerance for daily drops, and how much you value handsoff treatment.
Checklist for Your Next Appointment
- Ask if my IOP fluctuations are within safe limits.
- Discuss the potential benefit of a lowdose prostaglandin drop.
- Inquire about SLT as a next step if drops arent enough.
- Bring a list of systemic conditions (e.g., sleep apnea, hypertension).
- Ask about visualfield testing frequency and any new imaging options.
Conclusion
Even though the numbers on the tonometer may look normal, normaltension glaucoma still needs proactive care. Starting with prostaglandin eye drops, moving to laser if needed, and reserving surgery for advanced cases gives you a roadmap that many ophthalmologists recommend. Pair these medical steps with healthy lifestyle habits, regular monitoring, and open conversations with your eyecare team, and youll give your optic nerve the best shot at staying strong for years to come. If youve tried any of these treatments or have questions about your own plan, feel free to share your experience in the comments were all in this together.
FAQs
What is the main goal of treatment for glaucoma with normal eye pressure?
The primary goal is to lower intraocular pressure (IOP) from baseline to slow or stop optic nerve damage and preserve vision, even if IOP is within the normal range.
What medications are commonly used to treat normal-tension glaucoma?
Prostaglandin analog eye drops are first-line treatments to increase fluid outflow and reduce IOP by 25-30%. Additional options include alpha-2 agonists and carbonic anhydrase inhibitors.
How does selective laser trabeculoplasty (SLT) help in normal-tension glaucoma?
SLT targets pigmented cells in the drainage meshwork to improve fluid outflow, lowering IOP by about 15-20% without surgery or incisions.
When is surgery considered for normal-tension glaucoma?
Surgery such as trabeculectomy or tube-shunt implants is considered if medications and laser treatments fail to control disease progression or lower IOP sufficiently.
Are lifestyle changes important in managing normal-tension glaucoma?
Yes, improving cardiovascular health, managing systemic conditions, and regular monitoring complement medical treatment to support optic nerve health.