Heres the complete thyroid medications list youve been looking for from the mostprescribed synthetic levothyroxine to naturaldesiccated extracts, plus the key uses, typical dosages, and the sideeffects you should keep an eye on.
Whether youre dealing with hypothyroidism, hyperthyroidism, or just curious about a T3 boost, this guide shows which drug fits each condition, how they differ, and what women especially need to know about risks.
Why Knowledge Matters
Understanding the thyroid medications list isnt just academic; its a practical tool that can prevent months of trialanderror, costly lab work, and unnecessary frustration. When you know which pill does what, you can have a clearer conversation with your doctor and feel more confident about the treatment plan.
Who benefits? New patients, women planning pregnancy, caregivers, and even seasoned clinicians who need a quick reference. The information below balances the benefits of each drug with its potential downsides especially the patients.
RealWorld Example
Take Anna, a 34yearold teacher diagnosed with Hashimotos. She started on levothyroxine but kept feeling sluggish because the dose was off. By consulting a detailed thyroid medications list, she and her endocrinologist switched to a different brand and finetuned the dosage, finally feeling like herself again.
Drug Classification Overview
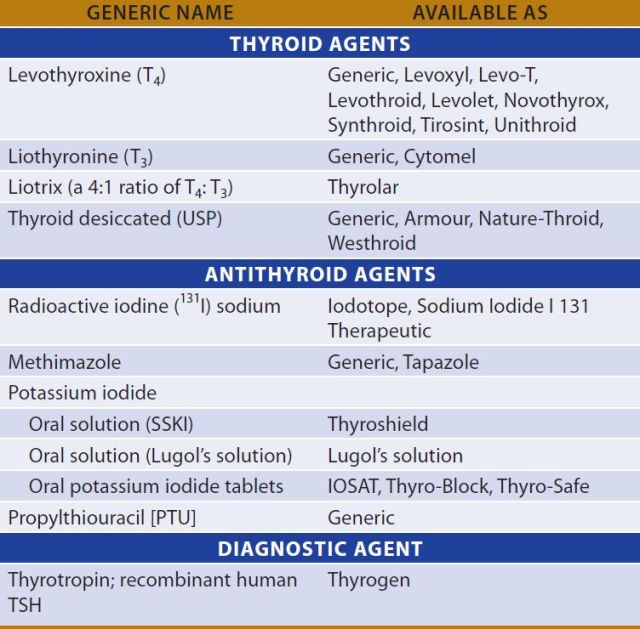
Thyroid drugs fall into a few major families. Below is a quick snapshot, followed by deeper dives into each category.
| Brand | Generic | Type | Typical Use | Common SideEffects |
|---|---|---|---|---|
| Synthroid | Levothyroxine | Synthetic T4 | Primary hypothyroidism | Weight gain, bone loss (women) |
| Cytomel | Liothyronine | Synthetic T3 | Rapid T3 boost, adjunct therapy | Palpitations, insomnia |
| Thyrolar | Liotrix | Combined T4/T3 | Refractory hypothyroidism | Heart rhythm changes |
| Armour Thyroid | Desiccated thyroid | Natural extract | Alternative to synthetic | Allergic reactions, variable potency |
Synthetic T4Only Medications
The workhorse of the list is levothyroxine (brand names like Synthroid, Levoxyl, Euthyrox, Unithroid). Its a synthetic form of thyroxine (T4) and is considered the best medicine for hypothyroidism by the American Thyroid Association. Typical adult doses range from 25g to 200g daily, adjusted based on TSH levels.
Why does levothyroxine dominate? Its stable, has a long halflife, and mimics the hormone your thyroid cant produce. Most patients achieve normal TSH within 68 weeks of starting treatment.
Synthetic T3Only Medications
Liothyronine (Cytomel) delivers pure triiodothyronine (T3). Its used when a rapid increase in thyroid activity is neededlike during pregnancy, when T3 conversion may be impaired, or as an addon for patients who dont feel fully better on T4 alone.
Because T3 has a shorter halflife, dosing is usually split (e.g., 25g twice daily). Watch out for faster heart rate and jittery feelings; these are classic concerns.
Combined T4/T3 Preparations
Liotrix (Thyrolar) blends T4 and T3 in a 4:1 ratio. Its less common but can help those who need a modest T3 boost without the peaks and valleys of pure liothyronine. Doses are often measured in micrograms (e.g., 50g/12.5g). Clinical evidence is mixed, so discuss this option with a specialist.
Natural/Desiccated Thyroid Extracts
Products like Armour Thyroid, NatureThyroid, Westhroid, and NP Thyroid use dried animal thyroid tissue, delivering both T4 and T3 in a fixed ratio. Some patients swear by them because they feel more natural, but the FDA warns that potency can vary batchtobatch, making dose titration tricky ().
ConditionSpecific Medications
Not every thyroid drug is for every condition. Lets match the right tools to the problem.
Best Medicine for Hypothyroidism
Levothyroxine remains firstline for most adults. Guidelines from the Endocrine Society suggest starting low (e.g., 2550g) for seniors or those with heart disease, then titrating up. Combination therapy (adding liothyronine) is considered only when patients remain symptomatic despite normal TSH.
Thyroid Medication List for Hyperthyroidism
When the thyroid is overactive, we flip the script. Antithyroid drugsmethimazole (Tapazole) and propylthiouracil (PTU)inhibit hormone synthesis. Methimazole is preferred for most adults, while PTU is reserved for the first trimester of pregnancy because of its slightly safer profile for the fetus.
Typical doses: methimazole 1030mg daily, PTU 50150mg daily. Sideeffects can include rash, liver enzyme elevation, and, rarely, agranulocytosis (a dangerous drop in white blood cells).
T3Focused Therapies & When to Use Them
If youre a woman trying to conceive, your doctor may add a low dose of liothyronine to ensure adequate T3 for the developing baby. Similarly, patients with deiodinase deficiency (trouble converting T4 to T3) often benefit from a T3 supplement.
Patient Story
Mike, 45, was on methimazole for Graves disease but developed liver enzyme spikes. His endocrinologist switched him to PTU, monitoring labs closely. Within weeks, his liver numbers normalized and his hyperthyroid symptoms stayed under control.
Side Effects & Safety
Every medication carries risks. Understanding them helps you spot problems early and discuss adjustments with your doctor.
Common SideEffects Across the List
- Weight changes (gain with T4, loss with T3)
- Menstrual irregularities especially with levothyroxine dose changes
- Hair thinning or increased shedding
- Fatigue or nervousness depending on over or underreplacement
Serious Risks & Red Flags
High doses of levothyroxine can lead to heart palpitations, atrial fibrillation, or bone loss (osteoporosis) concerns that are heightened in postmenopausal women. Antithyroid drugs may cause liver toxicity (especially PTU) or severe allergic reactions.
Monitoring Checklist
Keep this list handy when youre on any thyroid medication:
- TSH, Free T4, and Free T3 labs every 68weeks after a dose change, then every 612months once stable.
- Bone density scan (DEXA) for women >50years on longterm T4 therapy.
- Pregnancy test before starting therapy if youre of childbearing age.
- Watch for symptoms: rapid heartbeat, unexplained weight loss, severe mood swings, or jaundice (yellow skin/eyes).
Choosing the Right Med
Finding the perfect match feels a bit like trying on shoes you might need a few attempts before they feel just right.
Factors to Evaluate
- Diagnosis: Hypothyroidism vs. hyperthyroidism.
- Age & Gender: Women, especially during pregnancy, may need tighter dose control.
- Comorbidities: Heart disease, liver issues, or osteoporosis influence drug choice.
- Insurance & Cost: Generic levothyroxine is often covered, while desiccated extracts can be pricey.
Questions to Ask Your Provider
Dont be shy a good conversation can save months of guesswork.
- Which brand of levothyroxine has the most consistent potency?
- Do I need a T3 supplement, or will T4 alone suffice?
- How often should we check my labs, especially if Im a woman over 40?
- What should I do if I notice new symptoms after a dosage change?
DecisionTree Flowchart
Start: Diagnosed with a thyroid disorder? If hypothyroidism Is T4only working? Yes: stay on levothyroxine. No: consider adding liothyronine or switch to combined therapy.
If hyperthyroidism Choose methimazole (firstline) Any liver issues? Switch to PTU if needed.
Conclusion
Now you have a clear, organized thyroid medications list that covers synthetic T4 and T3 drugs, combined preparations, natural extracts, and antithyroid agents. Remember, the best medicine for hypothyroidism is usually levothyroxine, but personal factorsespecially for womenmay push you toward combination therapy or a desiccated product.
Balancing benefits and risks, staying on top of lab monitoring, and having open conversations with your healthcare provider are the keys to feeling your best. If youve tried a medication that didnt click, or youve discovered a sideeffect that surprised you, share your story in the comments. Your experience could help someone else find their perfect match.
Got questions? Drop them below, and lets keep the conversation going. Your thyroid health matters and together we can navigate it with confidence and compassion. For more on common medication risks and when to watch for them, see the guidance on drug safety warnings which can help you recognize serious drug side effects early.
FAQs
What is the best medication for hypothyroidism?
Levothyroxine (synthetic T4) is considered the first‑line treatment for most patients with hypothyroidism because it provides stable, long‑acting hormone replacement.
Can I take a natural desiccated thyroid extract instead of synthetic pills?
Natural extracts like Armour Thyroid contain both T4 and T3, but their potency can vary between batches. They may work for some people, but dosing is less predictable and they require careful monitoring.
When is liothyronine (Cytomel) used?
Liothyronine provides a rapid T3 boost and is often added for patients who don’t feel fully better on T4 alone, for women trying to conceive, or when conversion of T4 to T3 is impaired.
What are the common side‑effects of antithyroid drugs?
Antithyroid medications such as methimazole and PTU can cause rash, liver enzyme elevations, and, in rare cases, agranulocytosis (a severe drop in white blood cells).
How often should thyroid labs be checked after starting a new medication?
TSH, Free T4, and Free T3 should be rechecked every 6‑8 weeks after any dose change, then every 6‑12 months once stable.