Quick Answer Snapshot
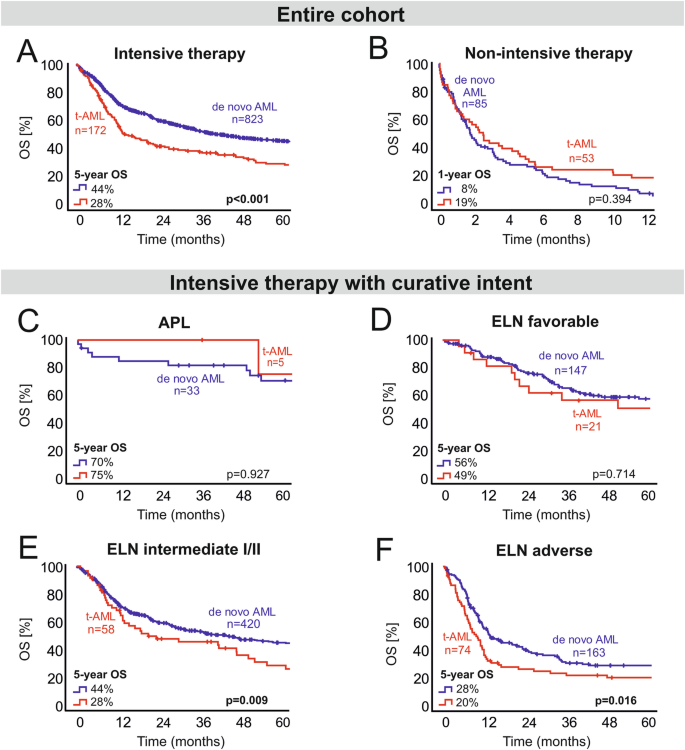
If youve just heard the term therapyrelated AML (tAML) and are wondering how long someone might live, the quick answer is: on average, about 1314 months with intensive chemotherapy and roughly 9 months with lessintensive regimens. These numbers come from largescale studies that compare tAML to denovo AML, which typically shows a median overall survival of around 40 months. Keep in mind, though, that every patient is unique age, specific genetic changes, and the type of treatment chosen can swing the odds dramatically.
Key Prognostic Factors
Understanding why the outlook varies is the first step to feeling a bit more in control. Below are the biggest drivers of prognosis in tAML:
Age and Overall Health
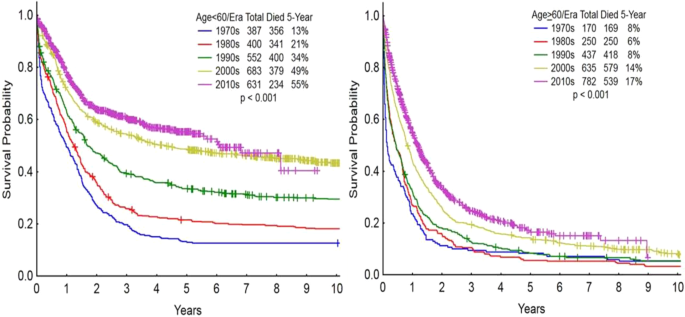
Patients over 60 years old, or those with other serious illnesses, usually have a shorter life expectancy. This isnt because the leukemia is magically more aggressive, but because the bodys ability to tolerate intensive therapy declines with age.
Cytogenetic Abnormalities
Cytogenetics the study of chromosome changes is a heavyweight in the prognosis game. Certain patterns, like the loss of chromosomes 5 or 7 or a complex karyotype (three or more unrelated chromosomal abnormalities), are linked to poorer outcomes.
| Abnormality | Prognostic Impact |
|---|---|
| Complex Karyotype | Very poor median OS < 6months |
| Monosomal Karyotype | Poor median OS ~ 8months |
| Loss of 5q/7q | High risk median OS ~ 9months |
| Normal Cytogenetics | Better median OS ~ 14months |
Gene Mutations That Matter
The genetic cheat sheet of each leukemia cell tells a story a lot beyond what chromosomes can show. In tAML, mutations in TP53, ASXL1, RUNX1, and DNMT3A are especially common and are associated with the shortest survivals. TP53mutated disease, in particular, often means the median overall survival drops below six months.
Latency Period
How long ago the original cancer treatment happened matters, too. A short latency less than two years after the first chemo or radiation usually points to a more aggressive leukemia, often with TP53 mutations. Longer latency periods tend to involve different cytogenetic patterns.
Treatment Options Impact
Now that you know the why, lets talk about the what. The treatment path you (or a loved one) choose can reshape the statistical picture.
Intensive Chemotherapy (7+3)
The classic 7+3 regimen seven days of cytarabine plus three days of an anthracycline remains a cornerstone for younger, fitter patients. In tAML, studies show a median overall survival of about 13.7months when this approach is used. Its aggressive, it can be brutal, but for many it offers the best chance at a durable remission.
Hypomethylating Agents with Venetoclax
When a patient cant tolerate the classic 7+3, doctors often turn to hypomethylating agents (HMAs) like azacitidine or decitabine, sometimes combined with the Bcell lymphoma2 inhibitor venetoclax. The combo has become a gamechanger, nudging median survival up by a couple of months compared with HMA alone. A recent trial reported a median OS of roughly 11months for this pairing in tAML patients who werent eligible for intensive therapy.
Allogeneic Hematopoietic Cell Transplant (HCT)
If you make it past the initial therapy and are a transplant candidate, HCT offers the strongest chance for longterm survival. According to data published in , about 48% of transplanteligible tAML patients are alive five years later. Thats a huge jump from the 1017% fiveyear survival seen with chemotherapy alone.
Targeted Therapies and Clinical Trials
New drugs that home in on specific mutations (e.g., FLT3 inhibitors for FLT3mutated disease, IDH1/2 inhibitors for IDHmutated cases) are creeping into the tAML arena. While the data are still early, earlyphase studies suggest modest survival gains, often in the range of 24 extra months. For many, the best option is to enroll in a clinical trial you get cuttingedge care and help move the science forward.
Special Patient Groups
Therapyrelated AML isnt a onesizefitsall condition. Two groups deserve special attention: children and those whose original therapy was a specific class of drugs.
Kids and tAML
Therapyrelated AML in children is rare less than 5% of all pediatric AML cases but when it does happen its usually tied to previous exposure to alkylating agents or radiation. Because children have a higher capacity to tolerate intensive regimens, the approach often mirrors adult intensive therapy, followed quickly by transplant when a suitable donor is found. The prognosis can be better than in older adults, but its still heavily dependent on the same genetic markers.
Alkylators vs. TopoisomeraseII Inhibitors
Two major culprits behind tAML are alkylating agents (like cyclophosphamide) and topoisomeraseII inhibitors (like etoposide). Alkylatorrelated disease usually shows up 510 years after exposure and often carries loss of chromosomes 5 and 7. TopoisomeraseIIrelated AML appears sooner (13 years) and is more frequently associated with TP53 mutations. Knowing which drug class preceded the leukemia helps doctors anticipate the likely cytogenetic profile and tailor therapy accordingly.
ICD10 Coding Matters
From a practical standpoint, the ICD10 code for therapyrelated AML is C92.0. Accurate coding isnt just bureaucracy it feeds national cancer registries, influences insurance reimbursement, and ultimately steers research funding. If youre navigating the healthcare system, making sure the correct code is used can smooth the path to getting the right treatment and support services.
How to Read Prognosis
When your oncologist hands you a pathology report, it can look like a foreign language. Lets demystify it together.
Decoding Mutations and Cytogenetics
Think of the report as a report card for the leukemia cells. Complex karyotype means the cells have multiple chromosomal mistakes thats a red flag. A listed TP53 mutation? Thats another warning sign. Conversely, normal cytogenetics is good news, suggesting a slightly better outlook.
Questions to Ask Your Doctor
- What is my ageadjusted risk category?
- Which mutations does my disease have, and how do they affect treatment choices?
- Am I a candidate for allogeneic transplant?
- Are there any clinical trials that match my profile?
- How will my prior cancer treatment (type and dose) influence my current plan?
Lifestyle Tweaks That Matter
While you cant change the genetics, you can optimize the rest. Good nutrition, staying uptodate on vaccinations, diligent infection prophylaxis, and psychosocial support (think counseling or support groups) have all been linked to modest improvements in quality of life and sometimes even survival. Think of it as giving your body the best possible fuel while the medical team does the heavy lifting.
Reliable Sources & Reading
When you start digging deeper, youll find a lot of technical papers. Here are a few trustworthy places to begin:
Conclusion
Therapyrelated AML carries a tougher prognosis than denovo disease, but the story isnt set in stone. Age, specific chromosome changes, and key gene mutations shape the odds, while the right blend of intensive chemotherapy, modern hypomethylating agents, transplant, and emerging targeted drugs can tip the balance toward a longer, fuller life. Remember, statistics are averages; individual journeys can diverge widely. Stay inquisitive, ask the right questions, and dont shy away from clinical trials theyre often the fastest lane to new hope. If anything feels overwhelming, reach out, share your worries, and lets navigate this together. Whats on your mind right now? Feel free to comment or ask for clarification were all in this conversation together.
For readers also interested in cancer nutrition during treatment, consider practical dietary strategies shown to support patients undergoing therapy; an overview on designing a supportive Cancer diet plan can be helpful when planning meals to maintain strength during intensive treatment.
FAQs
What is therapy‑related AML?
Therapy‑related AML (t‑AML) is a type of acute myeloid leukemia that develops as a late complication of previous chemotherapy, radiation, or both for an earlier cancer.
How long do patients with t‑AML typically survive?
On average, median overall survival is about 13–14 months after intensive chemotherapy and roughly 9 months with lower‑intensity regimens; outcomes improve with transplant or newer targeted therapies.
Which factors most affect the prognosis of t‑AML?
Key prognostic drivers are age and performance status, cytogenetic abnormalities (e.g., loss of 5q/7q, complex karyotype), high‑risk gene mutations such as TP53, latency period after the initial therapy, and eligibility for allogeneic transplant.
What treatment options offer the best chance of longer survival?
Intensive “7+3” chemotherapy, hypomethylating agents combined with venetoclax, and allogeneic hematopoietic cell transplantation are the main approaches that have shown the greatest survival benefit in t‑AML.
Is stem‑cell transplant a realistic option for most t‑AML patients?
Transplant is offered to patients who achieve remission and have an acceptable performance status; about 48 % of transplant‑eligible t‑AML patients remain alive at five years, compared with <10 % with chemotherapy alone.