Imagine you've just finished a tough round of chemotherapy or radiation and you're feeling relievedmaybe even hopefulbecause the primary cancer is finally under control. Then a question sneaks in: Could the very treatment that saved me later cause a new blood cancer? The short answer is yes. Certain drugs and radiation can damage the DNA in your blood-forming cells, setting the stage for therapy-related acute myeloid leukemia (tAML). But not everyone who gets chemo or radiation develops tAML; the risk depends on the specific agents, the total dose, and your own genetic makeup.
Below we'll walk through the exact therapy-related AML causes, look at the typical genetic fingerprints, explore how doctors diagnose and treat it, and give you practical tips on monitoring and prevention. Let's dive inno fluff, just the facts you need to understand both the benefits and the risks of lifesaving therapy.
What Is tAML
tAML, short for therapy-related acute myeloid leukemia, is a form of AML that appears after exposure to DNA-damaging cancer treatments. The World Health Organization classifies it separately from de-novo AML because its origins are tied to prior therapy. It typically shows up years after the original treatment, and its biology often looks tougherfor example, it frequently carries chromosome 5 or 7 deletions and TP53 mutations.
Although tAML represents only about 15% of all AML cases, its impact is significant because survivors of other cancers suddenly face a new, aggressive disease. The latency period varies: 13 years after topoisomerase-II inhibitors, and 37 years after alkylating agents.
| Feature | Typical Value | Source |
|---|---|---|
| Median latency (alkylators) | 37 years | |
| 5-year survival (tAML) | 2030% |
Core Causes
DNA-Damaging Chemotherapy Agents
Two families of chemo drugs are the main culprits:
- Alkylating agents (e.g., cyclophosphamide, melphalan, busulfan)they crosslink DNA strands, creating breaks that can misrepair into mutations. These agents usually lead to a longer latency period and are often linked with loss of chromosomes 5 and 7.
- Topoisomerase-II inhibitors (e.g., etoposide, anthracyclines)they interfere with the enzyme that untangles DNA during cell division, causing double-strand breaks. The resulting leukemia tends to appear sooner and often carries MLL/KMT2A gene rearrangements.
An oncologist I once chatted with explained that the mechanism matters. Alkylators scramble the DNA-code like an overenthusiastic editor, while topoisomerase inhibitors rip the pages out entirely. Both can ultimately trigger a malignant clone, just in slightly different ways.
Radiation Therapy
Whole-body or high-dose localized radiation can also set off tAML. The risk rises with total dose and when radiation is combined with chemotherapythink of it as adding gasoline to a fire.
Combined Modality & Cumulative Dose
Many patients receive both chemo and radiation, especially before a stem-cell transplant. When the cumulative exposure is high, the odds of DNA mishaps go up dramatically. For instance, a regimen that pairs high-dose busulfan with total-body irradiation is notorious for tAML in transplant survivors.
Patient-Specific Modifiers
- Ageolder bone marrow cells are less able to repair DNA.
- Genetic predispositioninherited DNA-repair defects (e.g., TP53, BRCA) amplify risk. For patients concerned about cancer risk factors, genetic testing can be a valuable tool in assessing overall risk and guiding monitoring strategies.
- Pre-existing myelodysplastic syndrome (MDS)a pre-leukemic condition that can be nudged over the edge.
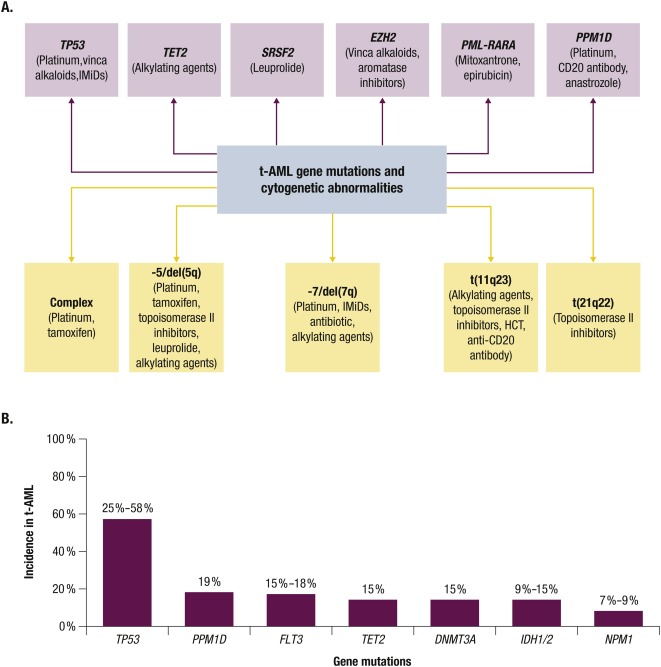
Cytogenetic Hallmarks
When doctors analyze the leukemia cells, they often see patterns that hint at a therapy-related origin.
Typical Chromosomal Abnormalities
Loss of chromosome 5 (5) or 7 (7) is classic, as is a complex karyotype involving three or more abnormalities. These changes are associated with poorer outcomes.
Common Driver Mutations
- TP53the most frequent mutation in tAML and a red flag for aggressive disease.
- RUNX1, ASXL1, NRAS/KRASalso show up, though less consistently.
- MLL/KMT2A rearrangementsoften linked to prior topoisomerase-II inhibitor use.
How Cytogenetics Shape Prognosis
Patients with TP53 loss or a complex karyotype tend to have a median overall survival of under 12 months, while those with more favorable profiles may survive longer. This is why current guidelines emphasize early cytogenetic testing.
Clinical Presentation
tAML often masquerades as ordinary fatigue or bruising, but there are a few telltale signs.
Common Symptoms
- Unexplained fatigue or weakness.
- Easy bruising or frequent nosebleeds.
- Recurrent infections due to low white cells.
- Shortness of breath from anemia.
Diagnostic Pathway
- Blood workCBC shows anemia, thrombocytopenia, and blasts.
- Bone-marrow biopsyessential for confirming AML and assessing blast percentage.
- Flow cytometrytypically CD34+, CD13+, CD33+.
- Cytogenetic & molecular testinglooks for the chromosome 5/7 loss, TP53, etc.
ICD-10 Coding
The official code for AML, including therapy-related cases, is C92.0. Using the correct coding helps with insurance and epidemiologic tracking.
Prognosis & Life Expectancy
Prognosis is a word that can feel heavy, so let's break it down into digestible pieces.
Key Survival Factors
- Age and overall health.
- Specific cytogenetic abnormalities (TP53 = poorer outlook).
- Response to initial induction therapy.
- Eligibility for allogeneic stem-cell transplant.
Median Overall Survival
For the average tAML patient, median survival hovers around 1224 months. By contrast, de-novo AML patients often reach 3040 months, reflecting the added genetic burden in therapy-related cases.
Life Expectancy Compared to De-Novo AML
Studies published in show a roughly 15-percentage-point drop in 5-year survival for tAML. The takeaway? Early detection and aggressive treatment are even more crucial.
Management Strategies
Balancing the desire to cure with the need to avoid further toxicity can feel like walking a tightrope. Here's how doctors typically navigate it.
Standard Induction: 7+3
The classic regimen combines seven days of continuous cytarabine with three days of an anthracycline. For tAML patients with TP53 mutations, oncologists may lower the anthracycline dose to reduce heart stress while still aiming for remission.
Targeted & Novel Therapies
- Venetoclax + hypomethylating agentsrecent phase II trials show promising remission rates in older or unfit patients.
- FLT3 inhibitors (e.g., midostaurin) when FLT3-ITD mutations appear.
- CAR-T and bispecific antibodiesstill experimental for AML but an exciting frontier.
Allogeneic Stem-Cell Transplant
If you're under 65 and have a suitable donor, transplant offers the best chance of long-term cure. The graft-versus-leukemia effect can eradicate residual disease, but the procedure carries its own risks (graft-versus-host disease, infections).
Supportive Care & Clinical Trials
Blood product support, infection prophylaxis, and psychosocial counseling are vital. And because tAML is rare, enrolling in a clinical trial often gives access to cutting-edge therapies and contributes to the scientific understanding of the disease.
Specific Populations
Children & Adolescents
Therapy-related AML is less common in kids, but when it occursoften after treatment for acute lymphoblastic leukemia with etoposidethe disease can be especially aggressive. Pediatric protocols usually involve lower-intensity chemotherapy followed by early transplant if possible.
Elderly Patients
Older survivors of solid tumors face higher baseline risk due to age-related DNA repair decline. Low-dose hypomethylating agents plus venetoclax have become a go-to regimen because it balances efficacy with tolerability.
Survivors of Specific Cancers
Examples include:
- Breast cancer patients treated with high-dose cyclophosphamide.
- Testicular cancer survivors who received multiple cycles of etoposide.
- Lymphoma patients exposed to CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone).
Prevention & Monitoring
How Oncologists Minimize Risk
Modern treatment plans often aim to spare DNA where possibleusing targeted therapies instead of broad-spectrum chemo, lowering cumulative alkylator doses, or opting for proton beam radiation that reduces off-target exposure.
Surveillance Recommendations
After high-risk therapy, the American Cancer Society suggests a complete blood count (CBC) every 36 months for at least five years. Any unexplained drop in blood counts should prompt a bone-marrow evaluation.
Patient Checklist
- Know the exact chemo agents and total doses you received.
- Schedule regular CBCs and keep a log of results.
- Report persistent fatigue, bruising, or infections to your doctor promptly.
- Discuss the possibility of DNA testing if you have a strong family history of blood cancers.
Key Takeaways
Therapy-related AML arises primarily from high-dose alkylating agents, topoisomerase-II inhibitors, and radiationoften years after treatment. Its cytogenetic fingerprint (loss of chromosomes 5/7, TP53 mutations) drives a tougher prognosis than de-novo AML. Early surveillance, prompt diagnosis, and an aggressive treatment plan (including possible transplant) give the best chance at survival. Most importantly, open conversations with your oncologist about risk-reduction strategies and follow-up schedules empower you to act quickly if warning signs appear.
If you've been through cancer treatment and this information resonates, consider sharing your story in the comments or reaching out to a support group. You're not alone, and together we can turn knowledge into action.
FAQs
Which chemotherapy agents are most commonly linked to therapy‑related AML?
Alkylating agents (e.g., cyclophosphamide, melphalan, busulfan) and topoisomerase II inhibitors (e.g., etoposide, anthracyclines) are the primary culprits.
How does radiation therapy contribute to therapy‑related AML?
High‑dose or whole‑body radiation can damage DNA in hematopoietic cells; risk increases with total dose and when combined with chemotherapy.
What genetic changes are typical in therapy‑related AML?
Loss of chromosomes 5 or 7, complex karyotypes, and TP53 mutations are the most frequent cytogenetic abnormalities.
What is the usual latency period between treatment and onset of t‑AML?
Alkylating agents often show a latency of 3‑7 years, while topoisomerase II inhibitors may lead to leukemia within 1‑3 years.
How should survivors monitor themselves for early signs of t‑AML?
Regular CBC tests every 3‑6 months for at least five years, and prompt evaluation of persistent fatigue, bruising, or low blood counts.