Alright, lets cut straight to the chase. If youre wondering how cervical cancer is staged this year, the 2023 FIGO revision boils down to three big ideas: finer substages, nodal involvement now has its own places, and imaging rules have finally caught up with reality. In plain English, the new system tells doctors exactly how far the cancer has spread, which means treatment can be matched more precisely to the disease and thats huge for outcomes.
Below youll find a friendly walkthrough of everything the 2023 staging looks like, why those changes matter, how to use them in practice, and a few quick resources you can download right now. Think of it as a cheatsheet you can share with a loved one, a partner, or that coworker who asked, Whats new with FIGO staging?
What Changed 2023
What are the new stage subdivisions?
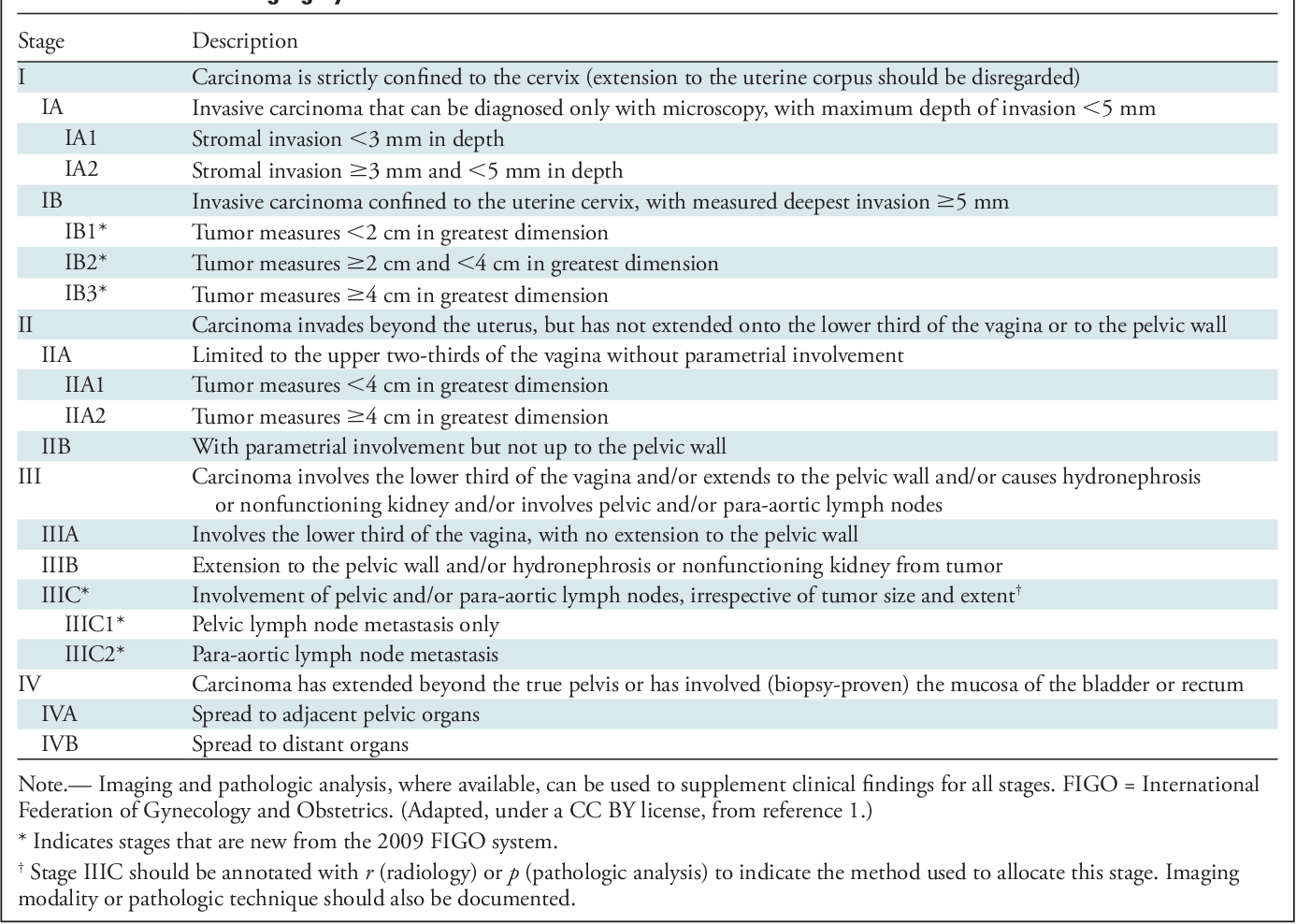
The 2023 FIGO update splits StageI into IA1, IA2, and IB1IB3, so we now have a more granular view of tumor size and depth of invasion. IA1 is a microscopic lesion less than3mm deep, IA2 jumps to 35mm, while IB1IB3 look at visible tumors ranging from 2cm up to >4cm.
StageI SubCategories (2023)
| Substage | Depth / Width | Clinical note |
|---|---|---|
| IA1 | 3mm depth, 7mm width | Usually eligible for cone excision |
| IA2 | 35mm depth, 7mm width | Often requires simple hysterectomy |
| IB1 | 2cm | Standard surgery or radiotherapy |
| IB2 | 24cm | Consider chemoradiation |
| IB3 | >4cm | Highrisk, multimodal approach |
How does nodal involvement get staged now?
Previously, lymphnode spread was hinted at in the narrative, but from 2023 it has its own clear categories:IIIC1 for pelvic node positivity andIIIC2 for paraaortic node positivity. This puts the spotlight on imaging and pathology findings that were, until now, tucked away in the footnotes.
NodeBased Staging Overview
- IIIC1 Cancer found in pelvic lymph nodes (common in FIGO StageIIIV disease).
- IIIC2 Cancer has reached paraaortic nodes, signaling a more advanced spread.
Which imaging modalities are officially accepted?
The 2023 revision finally gives a green light to MRI, PETCT, and even highresolution ultrasound when evaluating tumor size and nodal status. MRI remains the gold standard for softtissue detail, while PETCT shines for detecting distant nodal involvement. If youre reviewing treatment options and prognosis you may also find resources on related cancers and systemic therapies for example, summaries about anti-androgens prostate cancer can be useful when comparing systemic treatment approaches across tumor types.
Imaging Decision Tree
- Suspected early StageI? MRI is usually enough.
- Any concern for nodal disease? PETCT adds metabolic insight.
- Resourcelimited settings? Highresolution ultrasound can still provide valuable measurements.
Applying the Staging
Stepbystep: From biopsy to final stage
Heres the road map youll walk with your care team:
- Biopsy Confirms cervical cancer and provides histology.
- Clinical exam Looks at lesion size, vaginal involvement, parametrial spread.
- Imaging MRI for primary tumor, PETCT if nodes are suspected.
- Pathology review Depth of invasion, lymphvascular space invasion (LVSI).
- Staging assignment Combine all data into the FIGO 2023 label (e.g., IB2IIIC1).
When should I order an MRI vs. PETCT?
If youre dealing with a tumor thats still under 2cm and theres no clinical suspicion of spread, MRI alone will usually suffice. But once you suspect any nodal involvementsay, a palpable pelvic mass or a rising SCCAg leveladding a PETCT is a wise move. It may feel like extra testing, but catching a hidden node can change a treatment plan from surgery alone to combined chemoradiation, which can dramatically improve outcomes.
How to document stage in the EMR for billing?
Accurate coding is a lifesaver for both clinicians and patients. In the EMR, note the FIGO stage (e.g., StageIB2IIIC1) and pair it with the appropriate ICD10CM code (C53.9 for cervical cancer, plus Z85.41 for personal history when needed). A quick template looks like this:
Diagnosis: Cervical cancer, FIGO 2023 Stage IB2 IIIC1ICD10CM: C53.9Procedure: Radical hysterectomy with pelvic node dissectionNotes: MRI shows 3.2cm lesion, PETCT positive pelvic nodes
What common pitfalls lead to misstaging?
Weve all heard the it looked smaller on exam story. One realworld example: a 42yearold patient was initially staged IB2 based on clinical exam, but a PETCT later revealed paraaortic nodes, bumping her to IIIC2. The lesson? Never skip the imaging when theres any doubt; the new FIGO rules make it clear that nodal status cant be an afterthought.
StageSpecific Treatment
How does treatment differ between IA2 and IB1?
IA2 lesions are usually treated surgicallyeither a simple hysterectomy or a fertilitysparing cone if the patient wishes to preserve fertility. IB1, on the other hand, often calls for a radical hysterectomy or, for some women, primary radiotherapy if surgery isnt feasible.
Treatment Summary Table
| Stage | Preferred Treatment | FertilityPreserving Options |
|---|---|---|
| IA1 | Cone excision | Yes |
| IA2 | Simple hysterectomy | Limited (cone + lymph node assessment) |
| IB1 | Radical hysterectomy sentinel node biopsy | Rare, highly selected cases |
| IB2IB3 | Concurrent chemoradiation | No |
| IIIC1IIIC2 | Extended chemoradiation + possible brachytherapy | No |
What are the recommended therapies for IIIC1 vs. IIIC2?
Both categories get chemoradiation, but IIIC2 often requires an extended field to cover the paraaortic region. The typical regimen is weekly cisplatin with external beam radiotherapy (EBRT) to the pelvis and paraaortic nodes, followed by highdoserate (HDR) brachytherapy to the cervix itself.
Is fertility preservation still possible in early stages?
Yes, but only for very early disease (IA1, occasionally IA2). Options include a cone biopsy combined with sentinel node evaluation. The key is early detectionif the tumor has grown beyond 5mm depth, preserving the uterus becomes risky.
What is the prognosis associated with each stage?
Survival stats have improved thanks to the refined staging and tailored treatment. Roughly speaking, fiveyear overall survival (OS) looks like this:
- StageIA1IA2: >95%
- StageIB1: 8590%
- StageIB2IB3: 7080%
- StageIIIC1: 5565%
- StageIIIC2: 4055%
FAQs
What are the main changes in cervical cancer staging FIGO 2023?
The 2023 FIGO update introduces more detailed substages within Stage I, creates separate nodal involvement stages (IIIC1 for pelvic nodes and IIIC2 for paraaortic nodes), and officially includes MRI, PETCT, and high-resolution ultrasound in staging criteria.
How is nodal involvement staged in FIGO 2023?
Nodal involvement now has distinct categories: IIIC1 indicates cancer spread to pelvic lymph nodes, while IIIC2 indicates involvement of paraaortic lymph nodes, reflecting more advanced disease and guiding treatment intensity.
When should MRI versus PETCT be used in cervical cancer staging?
MRI is preferred for assessing tumor size and local extent, especially in suspected early-stage disease under 2 cm without nodal suspicion. PETCT is used when nodal involvement or more advanced spread is suspected to detect metabolic activity and distant nodes.
Is fertility preservation possible under FIGO 2023 staging?
Yes, fertility preservation is possible mainly in very early stages IA1 and sometimes IA2 through cone excision combined with sentinel lymph node evaluation, but risks increase with tumor depths beyond 5 mm.
How does FIGO 2023 staging impact treatment decisions?
The refined staging allows personalized treatment: smaller tumors (IA1, IA2) often undergo surgery alone, stages IB2 to IB3 typically receive chemoradiation, and nodal involvement stages (IIIC1, IIIC2) require extended chemoradiation with tailored radiation fields.