Quick Overview
Definition
Transcatheter Aortic Valve Implantation, or TAVI, is a catheterbased valve replacement. Instead of a big chest incision, a thin tube is slipped through a blood vessel (usually the femoral artery in the groin) and guided up to the heart where a new bioprosthetic valve is deployed.
How It Works
The new valve is made of animal tissue (cow or pig) mounted on a metal frame. Once it reaches the diseased native valve, it expands (either with a balloon or by selfexpansion) and pushes the old, calcified leaflets aside. The result is a fresh, functional valve that lets blood flow normally again.
Key Anatomy
- Aortic valve the door that controls blood flow from the heart to the body.
- Annulus the ring where the new valve sits.
- Access vessels typically the femoral artery, but alternatives include the subclavian or directaortic route.
Authority Note
According to the , TAVI is now a standard option for many patients with severe aortic stenosis, especially those considered highrisk for openheart surgery.
Good Candidate?
Eligibility Criteria
If youve been diagnosed with severe aortic stenosis and are over 65, or youre younger but have frailty or other health issues that make a sternotomy risky, youre likely a good candidate. Doctors will look at:
- Severity of valve narrowing (measured by echo or CT).
- Overall health and comorbidities (kidney function, lung disease, etc.).
- Vascular anatomy the arteries must be big enough to accommodate the delivery system.
Contraindications
Not everyone can have a TAVI. Situations that usually rule it out include active infections, unsuitable peripheral vessels, or a very young patient who would outlive the prosthetic valve.
RealWorld Example
Take Mary, 78, who struggled to climb stairs because her heart was squeezing blood through a calcified valve. After a thorough CT scan showed healthy femoral arteries, she qualified for TAVI and recovered at home in just a week. By contrast, her friend John, also 78, had severe peripheral artery disease, so his heart team recommended traditional surgery instead.
StepbyStep Walkthrough
Preop Preparation
Before the cath lab, youll undergo detailed imaging a CT scan to map the aorta and a transthoracic echo to gauge valve function. An anesthesiologist decides whether youll be lightly sedated or under general anesthesia. Medications that increase bleeding risk are typically paused.
Access Site & Catheter Insertion
The most common route is the femoral artery. After a small incision, a sheath (about the size of a garden hose) is inserted, and the catheter rides up through the aorta toward the heart. If the femoral route isnt viable, doctors may go through the subclavian artery (just beneath the collarbone) or even perform a directaortic approach.
Valve Positioning & Deployment
Two main valve types exist:
- Balloonexpandable: A balloon inflates to push the valve into place.
- Selfexpanding: The valve springs open on its own once positioned.
Fluoroscopy (realtime Xray) guides the doctor, ensuring the new valve sits just right. Once released, the old leaflets are pressed aside, and blood can flow freely again.
Postdeployment Assessment
Immediately after deployment, the team runs a quick echo and aortography to confirm proper valve function and check for leaks. Minor bleeding at the access site is common but usually stops on its own.
Recovery Room & Hospital Stay
Most patients spend a night or two in a cardiac care unit. If everything looks good, youll be moved to a regular floor and discharged within 24 days.
Video Resource
A clear from a leading heart center walks you through each step a helpful visual if youre a seeittobelieveit kind of person.
Procedure Cost
| Region | Average Cost (USD) | Whats Included? | Insurance Coverage |
|---|---|---|---|
| United States (private) | $45,000 $80,000 | Device, cath lab, hospital stay, imaging, followup | Most plans cover 7090% |
| United States (Medicare) | $30,000 $50,000 | Same as private | Full coverage after deductible |
| Australia (public) | AUD $30,000 $55,000 | Device, surgery, rehab | Government subsidised, outofpocket minimal |
Whats Included?
The price typically bundles the valve device (the most expensive item), the catheter lab time, anesthesia, imaging, postop monitoring, and the first followup echo.
Financial Assistance
If you have private insurance, check whether they consider TAVI medically necessary. Public health systems often have pathways for highrisk patients, and charities sometimes provide travel grants for those who need to go to a specialized centre.
Trust Signal
A recent breaks down the public funding model, confirming the figures above.
Recovery Timeline
First 24 Hours
Youll be in a monitored bed, watching your heart rhythm and blood pressure. Minor groin soreness is normal; a light analgesic usually does the trick.
First Week
Most patients are up and moving within a day. Light walking, gentle stretches, and avoiding heavy lifting are the rules of thumb. Your doctor will give you woundcare instructions for the tiny incision site.
First Month
This is when cardiac rehab kicks in. A physiotherapist will design a hearthealthy exercise plan, and youll have a followup echo around 30 days to confirm the valve is working perfectly.
LongTerm Lifestyle
- Stay on bloodthinners as prescribed (usually aspirin plus a second agent for a few months).
- Adopt a heartfriendly diet think plenty of veggies, lean proteins, and less salt.
- Keep regular checkups every 612 months.
Patient Story
Mark, 72, says, I was back gardening within a week. The scar was barely there, and I felt like I got a new lease on life. Real anecdotes like his make the recovery process feel tangible, not just a list of dates.
Risks & Complications
Common Risks
- Vascular injury at the access site (bleeding or artery damage).
- Conduction abnormalities about 1015% need a permanent pacemaker.
- Kidney strain from contrast dye.
Serious, Less Common Risks
- Stroke roughly 23% in most studies.
- Paravalvular leak (blood flowing around the new valve).
- Device malfunction or need for a second valve.
- Mortality 12% in contemporary lowrisk trials.
| Complication | Incidence (%) | Source |
|---|---|---|
| Major Vascular Complication | 46 | British Heart Foundation |
| Need for Pacemaker | 1015 | National Heart, Lung & Blood Institute |
| Stroke | 23 | JACC Clinical Trial 2023 |
Balanced View
Every procedure carries risk, but TAVIs minimallyinvasive nature often means a lower overall complication rate compared with traditional surgical aortic valve replacement (SAVR). The key is a thorough preprocedure evaluation and a heart team that tailors the approach to your anatomy.
Life Expectancy
Survival Data
Recent trials show encouraging numbers:
- 1year survival: ~90%.
- 5year survival: 7080% for lowrisk patients.
- 10year survival: approaching 60% in select groups.
Factors That Influence Longevity
Age, kidney function, and whether you need a permanent pacemaker are the biggest predictors. Also, the type of valve (balloonexpandable vs. selfexpanding) can affect durability, though both have shown good midterm performance.
Expert Commentary
Dr. Patel from notes, Patients who adhere to postprocedure rehab and medication regimens often enjoy a life expectancy close to their agematched peers.
TAVI vs TAVR
Terminology Clarification
Short answer: theyre the same thing. TAVI (Transcatheter Aortic Valve Implantation) is the term more common in Europe and Australia, while TAVR (Transcatheter Aortic Valve Replacement) is used predominantly in the United States. Both describe the catheterbased valve replacement.
Procedure Differences?
Theres none. The devices, techniques, and outcomes are identical; the distinction is purely branding.
Comparison Table
| Aspect | TAVI | TAVR |
|---|---|---|
| Geographic Usage | Europe, Australia, Asia | United States |
| Device Types | Same (balloon/selfexpanding) | Same |
| Clinical Outcomes | Equivalently high | Equivalently high |
Is TAVR Major Surgery?
Minimally Invasive vs OpenHeart
Traditional surgical aortic valve replacement (SAVR) requires a full sternotomy (splitting the breastbone) and often a heartlung machine. TAVR/TAVI is done through a small puncture, no chest opening, and usually without stopping the heart. Thats why many describe it as not a major surgery.
Patient Perception
Its normal to feel anxious. Major to a layperson often means big scar, long hospital stay. With TAVI, the scar is tiny, the stay is short, and recovery is swift. Still, the procedure isnt riskfree, so a candid conversation with your cardiologist is essential.
Surgeon Q&A
Dr. Liu, interventional cardiologist, says, I reassure patients by comparing TAVI to getting a stent in a coronary artery youre still fixing a lifethreatening problem, but the body isnt torn open.
BottomLine Resources
Find a Qualified Centre
Look for hospitals accredited by the or the local cardiac society. In Australia, the maintains a list of TAVIready facilities.
Prepare for Your First Appointment
- Bring a list of current medications (including overthecounter).
- Have recent imaging (echo, CT) if you have them.
- Write down questions e.g., What is my expected recovery timeline? or Will I need a pacemaker?
Further Reading & Tools
Useful links:
Download our printable recovery planner (PDF) from the pages sidebar to keep track of meds, appointments, and milestones.
Conclusion
A TAVI procedure gives patients with severe aortic stenosis a lessinvasive route to a new valve, delivering quicker recovery and comparable survival to openheart surgerywhile still carrying real risks you should weigh with your doctor. Understanding the steps, costs, recovery timeline, and longterm outlook empowers you to make an informed decision. Got more questions? Reach out to a heartfailure specialist or explore the resources above, and take the next step toward a healthier heart.
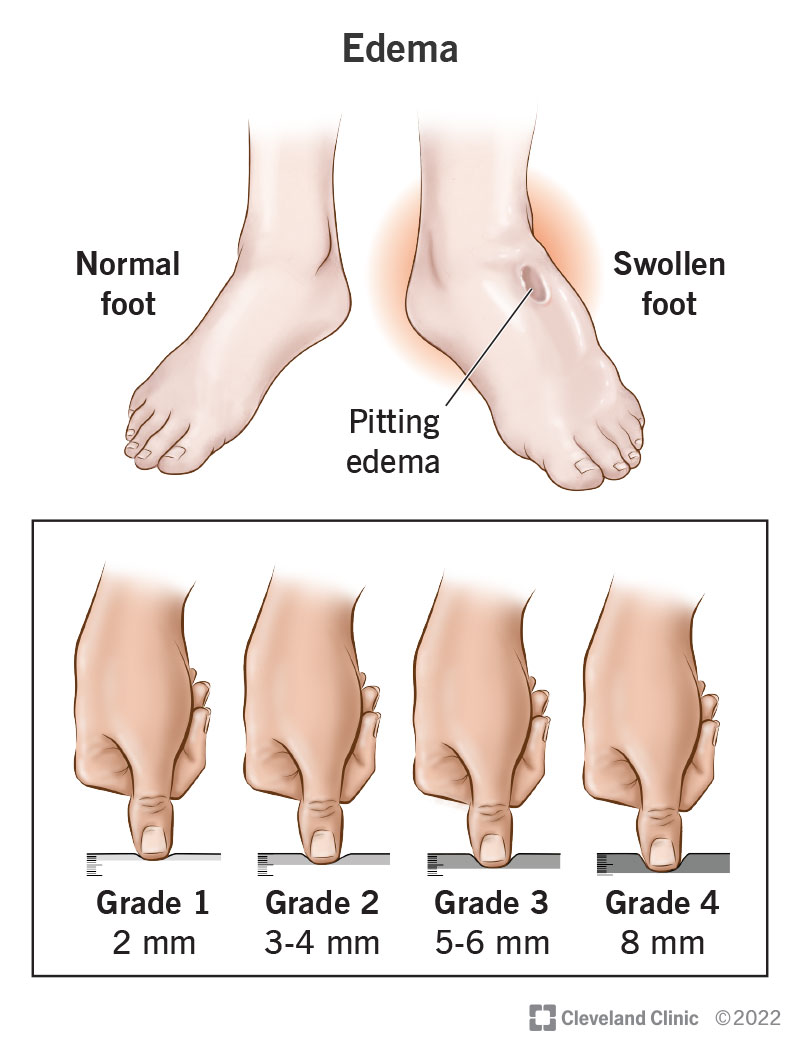
Patients experiencing swelling or fluid retention around the legs after heart procedures should be aware of common causes and treatments; for more on peripheral causes and management, see peripheral edema.
FAQs
What exactly is the TAVI procedure?
TAVI (Transcatheter Aortic Valve Implantation) is a minimally invasive method to replace a diseased aortic valve by delivering a new bioprosthetic valve via a catheter inserted through an artery, often the femoral artery, without opening the chest.
Who is a suitable candidate for TAVI?
Good candidates are typically patients over 65 with severe aortic stenosis or younger patients with comorbidities making open-heart surgery risky. Vascular anatomy and overall health are carefully evaluated before proceeding.
How long is the recovery time after a TAVI procedure?
Recovery is usually swift, with hospital stays between 2 to 4 days, most patients up and walking within a day, and cardiac rehab beginning within the first month to support heart health and function.
What are the common risks associated with TAVI?
Common risks include vascular injury at the access site, conduction issues requiring pacemaker implantation (10-15% cases), kidney strain from contrast dye, stroke (2-3%), and paravalvular leak. Serious complications are less common but possible.
Is TAVI the same as TAVR?
Yes, TAVI and TAVR are terms for the same procedure; TAVI is used more outside the U.S., while TAVR is common in the U.S. Both involve catheter-based aortic valve replacement with identical devices and outcomes.