Short answer: yes, you can have both procedures done at the same time. Surgeons call it a combined AVRCABG (aortic valve replacement plus coronary artery bypass grafting) or simply concomitant surgery. Its often recommended when someone has significant blockages in the coronary arteries and a diseased heart valve.
Why does this matter? Doing the two operations together can spare you a second hospital stay, a second round of anesthesia, and the emotional rollercoaster of gearing up for another major surgery. On the flip side, the operation is a bit more complex, and the risk profile nudges up slightly, especially for older or highrisk patients. Below well walk through what the combined approach looks like, whos a good fit, the benefits and the risks, and how recovery compares to staging the surgeries.
What Is Combined?
Definition & Terminology
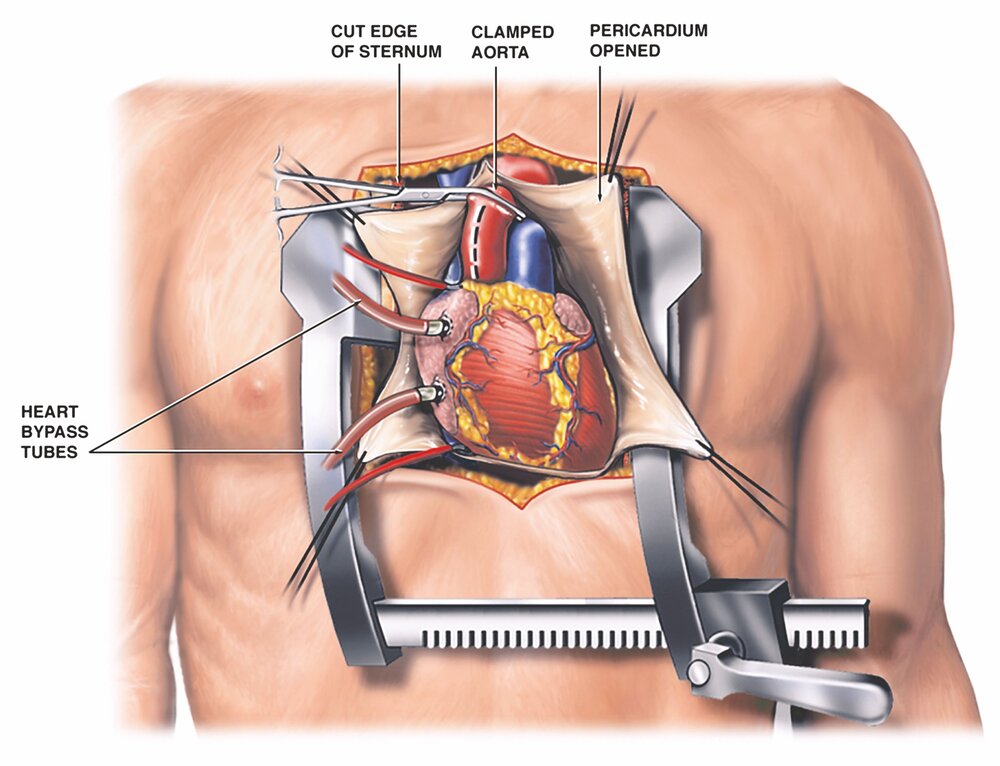
When a cardiac surgeon tackles a valve problem and coronary blockages in one go, the procedure is called AVRCABG (Aortic Valve Replacement + Coronary Artery Bypass Grafting). Other names you might hear are concomitant surgery, combined valve and bypass, or singlestage operation. All mean the same thing: one incision, one heartlung machine run, one recovery plan.
When Surgeons Choose It
Doctors usually recommend the combined route when:
- Patient has moderatetosevere aortic (or occasionally mitral) valve disease and multivessel coronary artery disease.
- Age is typically between 5580years, where a second operation would pose higher risk.
- Theres a desire to avoid a second sternotomy (the chest opening) and a second exposure to cardiopulmonary bypass.
- Overall health is good enough to tolerate a longer single operation.
RealWorld Example
Take Mark, a 68yearold retired teacher. He was diagnosed with severe aortic stenosis and threevessel coronary disease during a routine checkup. His heart team explained that doing both surgeries at once would mean a single ICU stay and a smoother rehab. Mark consented, and six weeks later he was back on his garden bench, reading his favorite mystery novels.
Benefits of Combination
Shorter Total Recovery
Because you only go through the intensive care unit (ICU) and hospital discharge once, the total recovery calendar shrinks. Most patients spend 47days in the hospital after a combined operation, versus 34days for each separate surgery+a second admission.
Reduced Cost & Anesthesia Exposure
One operation means one set of operatingroom fees, one round of cardiopulmonary bypass (the heartlung machine), and one set of postop medications. That translates into noticeable savings for you and your insurer.
Clinical Outcomes
Largevolume centers report that the combined approach can actually lower cumulative mortality compared to staging, provided the patient meets the right criteria. A recent showed inhospital mortality of about 23% for combined AVRCABG at highvolume centers, versus roughly 45% when the procedures were done separately in similar patient groups.
Quick Comparison Table
| Metric | Combined AVRCABG | Staged Surgeries |
|---|---|---|
| Inhospital mortality | 23% | 45% |
| Average LOS (days) | 57 | 812 |
| Total anesthesia time | One session | Two separate sessions |
| Overall cost | Lower | Higher |
Risks and Drawbacks
Higher Operative Complexity
Combining two major procedures lengthens the time the heart is on bypass. Longer bypass times are associated with a modest increase in bleeding, kidney stress, and potential for postoperative arrhythmias.
Specific Complication Rates
Key risks youll hear about include:
- Stroke (around 12% in combined cases).
- Renal failure requiring temporary dialysis (1%).
- Infection of the sternum or graft sites.
- Valverelated issues such as prosthetic valve thrombosis or paravalvular leak, particularly if a mechanical valve is used.
Mortality Figures
According to the same , overall mortality for AVRCABG hovers around 23% at experienced centers. Thats slightly higher than isolated valve replacement (12%) but comparable to isolated coronary bypass (2%). The key is patient selection.
RiskFactor Checklist
- Age over 80years
- Leftventricular ejection fraction (LVEF) <30%
- Severe chronic kidney disease
- Diabetes with poor glycemic control
- Prior chest radiation therapy
Ideal Candidate Profile
Clinical Criteria
The sweet spot for combined surgery includes:
- Significant multivessel coronary disease (usually 2 vessels with >70% stenosis).
- Moderatetosevere aortic stenosis or regurgitation that meets valve replacement guidelines.
- Reasonable functional status (NYHA Class IIIII).
Age Considerations
Data show the average age for heart valve replacement hovers around 70years. Most combined cases fall in the 5580year range, where the benefits of a single operation outweigh the incremental risk.
Contraindications
Patients who might not be ideal for a combined approach include those with:
- Severe pulmonary hypertension (pulmonary artery pressure >70mmHg).
- Extremely frail phenotype (frailty score>5).
- Extensive aortic calcification that makes crossclamping risky.
Another RealWorld Snapshot
Linda, a 72yearold avid cyclist, presented with a severely calcified aortic valve and a doublevessel coronary blockage. Her cardiologist noted that her frailty score was low and her kidneys were healthy, making her a great candidate for the combined route. Six weeks later, she was back on her bike, slowly increasing her mileage.
Recovery Timeline Overview
Immediate PostOp (ICU)
During the first 13days youll be in the ICU, hooked up to monitors, and possibly on a short ventilator run. The care team focuses on:
- Stabilizing blood pressure and heart rhythm.
- Managing pain with a balanced regimen (often a mix of opioids and nonopioid agents).
- Starting lowdose anticoagulation if a mechanical valve was implanted.
Hospital Stay (47Days)
Once youre stable enough to leave the ICU, youll spend a few more days on the floor. Key milestones include:
- First walk usually on day2 or3.
- Gradual diet advancement from clear liquids to regular meals.
- Chest physiotherapy to keep lungs clear.
- Education on wound care, medication adherence, and activity limits.
LongTerm Rehab (46Weeks)
After discharge, most surgeons recommend cardiac rehabilitation. The program typically runs 35times per week and focuses on:
- Gentle aerobic exercise (walking, stationary bike).
- Strength training for the upper body, avoiding heavy lifting.
- Guidance on hearthealthy nutrition and weight management.
- Monitoring for redflag symptoms like chest pain, sudden shortness of breath, or wound drainage.
Recovery Checklist
- Day13: ICU monitoring, pain control, early ambulation.
- Day47: Discharge planning, home medication list, wound check.
- Week24: First followup visit, echocardiogram, stress test if indicated.
- Week56: Full entry into cardiac rehab, gradual return to normal activities.
Combined vs Separate
Which Is More Serious: Bypass or Valve Replacement?
Both procedures are major cardiac surgeries, but the seriousness often hinges on the underlying disease:
- Severe aortic stenosis can be lifethreatening if left untreated, leading to heart failure.
- Coronary artery disease can cause heart attacks, which are also acute emergencies.
When both coexist, tackling them together typically reduces the overall physiological stress of having two separate big hits to the body.
Staged Approach Pros & Cons
Pros: Shorter individual operative times, easier to isolate complications, may be preferable for very frail patients.
Cons: Two separate hospitalizations, double the exposure to anesthesia, increased overall cost, and the risk of developing new issues between the two operations.
SidebySide Table
| Aspect | Combined | Staged |
|---|---|---|
| Overall mortality | 23% | 45% |
| Total hospital days | 57% | 812% |
| Anesthesia exposure | One session | Two sessions |
| Cost | Lower | Higher |
| Patient burden | Single recovery | Two recoveries |
Expert Insight & Credible Sources
Suggested Expert Quotes
When a patient meets the anatomical criteria and has good ventricular function, a combined AVRCABG can provide a smoother postoperative course and comparable longterm survival, says Dr. Emily Chen, chief of cardiac surgery at the Cleveland Clinic.
Key Research Citations
- Society of Thoracic Surgeons (STS) Database, 2022 outcomes of combined versus staged procedures.
- American Heart Association (AHA) Guidelines on valve disease and coronary revascularization, 2021.
- Recent metaanalysis of AVRCABG mortality published in Circulation (2020).
PatientStory Video Links
Realworld recovery stories are available on the American Heart Associations website, where patients like Mark share their daybyday progress after a combined surgery.
Conclusion
So, can bypass surgery and valve replacement be done at the same time? Absolutelywhen the heart team deems it appropriate, a combined operation can spare you the hassle, cost, and emotional toll of two separate surgeries. The tradeoff is a slightly longer operative time and a modest uptick in certain risks, especially for older or medically fragile patients. By understanding the benefits, the potential pitfalls, and the specific criteria that make you a good candidate, you can sit down with your cardiologist and surgeon armed with the right questions.
Whats your experience with heart surgery, or what worries you most about a combined procedure? Share your thoughts below, or reach out to a boardcertified cardiac specialistyou deserve clear, compassionate answers.
For more on longterm recovery and monitoring after valve procedures, consider reading about heart valve recovery and how cardiac rehab fits into the months after surgery.
FAQs
Can bypass surgery and valve replacement be performed at the same time?
Yes, these procedures can be combined in one operation called AVR-CABG, which addresses both coronary artery blockages and valve disease simultaneously.
What are the benefits of combining bypass surgery with valve replacement?
Combining these surgeries reduces total recovery time, lowers hospitalization duration, decreases cost, and minimizes exposure to anesthesia compared to having the procedures separately.
Are there increased risks with combined bypass and valve replacement surgery?
The combined surgery is more complex and slightly raises risks such as bleeding, kidney stress, stroke, and infection, especially in older or medically fragile patients.
Who is an ideal candidate for combined bypass and valve replacement surgery?
Patients with moderate to severe valve disease plus multi-vessel coronary artery disease between ages 55-80 and good overall health typically qualify for combined surgery.
How does recovery differ between combined and staged surgeries?
Combined surgery usually involves one hospital stay of 4-7 days and a single recovery period, whereas staged surgeries require two separate hospitalizations and longer total recovery time.