Hey there, friend. If youve landed on this page youre probably hunting for answers about pulmonary hypertension treatment and you dont have time to wade through endless medical jargon. Lets cut straight to the chase: there are solid, evidencebacked medicines that can keep the pressure in your lungs under control, exciting new therapies that might reshape the future, and lifestyle tweaks that truly support your heart. Below, Ill walk you through everything you need to know, sharing the good, the risky, and the realistic.
Grab a comfy seat, maybe a cup of tea, and lets dive into the options that can help you breathe easier today and tomorrow.
Quick Treatment Guide
FirstLine Medications You Should Know
The backbone of any pulmonary hypertension treatment plan is a handful of drug classes approved by the FDA and endorsed by the . Heres the rundown:
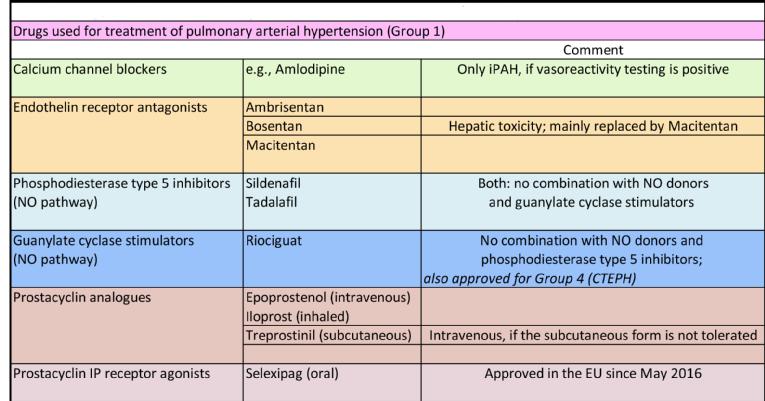
- Endothelinreceptor antagonists (ERAs) e.g., bosentan, ambrisentan. They block a hormone that tightens blood vessels.
- Phosphodiesterase5 inhibitors (PDE5i) sildenafil and tadalafil, the same family as Viagra but at a lower dose for the lungs.
- Soluble guanylate cyclase stimulators riociguat, a newer player that relaxes vessels from a different angle.
- Prostacyclin analogues epoprostenol (IV), treprostinil (subQ or inhaled). Theyre potent and usually reserved for more severe cases.
All of these have solid data behind them, and your doctor will choose based on your WHO functional class, sideeffect tolerance, and personal schedule.
When Supplemental Oxygen Helps
If your blood oxygen level dips below 90%, supplemental oxygen can ease the workload on your heart. Guidelinebased sources recommend aiming for 9295% saturation at rest and during activity. A simple nasal cannula often does the trick, and many patients notice less fatigue within a week.
CalciumChannel Blockers: The Miracle for Select Patients
About 10% of people with pulmonary hypertension respond dramatically to highdose calciumchannel blockers (CCBs). The secret? A vasoreactivity test during rightheart catheterisation. If youre a responder, a drug like amlodipine can lower pulmonary pressure by up to 30% in weekssome call it a miracle cure for the right reasons. But beware: nonresponders can suffer dangerous hypotension, so careful testing is a must.
Emerging Therapies Overview
Whats New in 2025?
Research never sleeps, and 2025 has already delivered some buzzworthy candidates:
- Sotatercept a ligand trap that rebalances the bonemarrowderived cells influencing vascular remodeling. Early phaseIII trials show a 45% reduction in clinical worsening.
- Imatinib (lowdose) originally a cancer drug, now being repurposed to target tyrosinekinase pathways that drive vessel thickening.
Both are still under regulatory review, but they give hope that future pulmonary hypertension treatment guidelines will broaden beyond the current trio of drug classes.
Is Pulmonary Endarterectomy Still the Only Cure?
For chronic thromboembolic pulmonary hypertension (CTEPH), pulmonary endarterectomy (PEA) remains the goldstandard surgical cure. Success rates at top centers hover around 85% with marked symptom relief. However, the procedure is technically demanding, carries risks like reperfusion injury, and isnt an option for everyone.
Inhaled vs. Subcutaneous Prostacyclins
Traditional IV prostacyclin is effective but cumbersome. Newer inhaled (e.g., iloprost) and subcutaneous (e.g., treprostinil) forms offer comparable hemodynamic benefits with fewer linerelated infections. Below is a quick comparison:
| Route | Convenience | Common SideEffects | Typical Candidates |
|---|---|---|---|
| IV (epoprostenol) | Requires pump & daily line care | Line infection, flush headaches | Severe PAH, refractory to oral meds |
| SubQ (treprostinil) | Portable pump, less line work | Site pain, bruising | Patients seeking homebased therapy |
| Inhaled (iloprost) | Handheld inhaler, 46 times daily | Cough, throat irritation | Those who can manage dosing schedule |
Lifestyle Tweaks That Complement Medicine
Even the best drug cocktail benefits from a supportive lifestyle. Think of your heart as a highperformance engineit runs smoother with premium fuel:
- Exercise Lowimpact activities (walking, stationary cycling) 34 times a week boost exercise capacity without overtaxing the right ventricle.
- Lowsalt diet Reduces fluid retention; aim for <2g sodium per day.
- Quit smoking Smoking narrows vessels further; cessation improves oxygenation immediately.
Natural Approaches Explained
Miracle Cure Myths Debunked
Its tempting to chase headlines promising a miracle cure for pulmonary hypertension. Sadly, most of those claims sprout from anecdotal reports or unverified supplements. No herb or fad diet has robust clinical evidence to replace approved drugs. When you hear something that sounds too good to be trueespecially if it suggests stopping your prescribed regimenpause and discuss it with a specialist.
Nutrition That May Support Your Therapy
Certain nutrients have modest, scientificallybacked benefits:
- Omega3 fatty acids Antiinflammatory; found in fatty fish, flaxseed.
- Larginine A precursor to nitric oxide, which helps vessels relax. A 2022 metaanalysis (cited in the ) showed modest improvement in exercise capacity when combined with standard therapy.
- Vitamin D Low levels correlate with worse outcomes; supplementation may aid overall cardiovascular health.
These foods are supportive, not substitutive. Always run new supplements by your doctor to avoid unwanted drug interactions.
When to Talk to Your Doctor About Alternative Therapies
Any alternative approach should be discussed before you start. Redflag signs include:
- Sudden drops in blood pressure after taking herbal extracts.
- New onset dizziness, palpitations, or swelling.
- Any suggestion to replace a proven medication with a natural option.
Open communication keeps your treatment safe and effective.
Choosing the Best Medication
Key Factors to Weigh
Deciding what is the best medication for pulmonary hypertension isnt a onesizefitsall answer. Consider:
- Disease severity (WHO functional class IIV).
- Comorbidities e.g., liver disease may steer you away from certain ERAs.
- Lifestyle Do you prefer a oncedaily pill or can you manage an infusion pump?
- Cost & access NHS formulary, insurance coverage, patient assistance programs.
Simple Decision Flowchart
Imagine a flowchart you could sketch on a napkin:
- Is vasoreactivity positive? Try highdose CCB.
- Are you WHO class IIIII? Start oral ERA or PDE5i (or combine).
- Severe (class IV) or refractory? Add prostacyclin analogue (IV/subQ) or consider combination therapy.
- Eligible for surgery? Evaluate for PEA or balloon pulmonary angioplasty.
Thats a simplified version, but it shows how clinicians blend guidelines with personal factors.
Monitoring Your Progress
Regular followup is vital. Typical schedule includes:
- 6month echocardiogram to assess rightventricular size.
- Annual rightheart catheterisation if symptoms change.
- Blood tests for liver function (ERAs) and kidney function (prostacyclins).
Staying on top of these checks helps catch sideeffects early and finetunes therapy.
RealWorld Experiences
Case Study: My Journey with Combination Therapy
Meet Alex, a 48yearold teacher diagnosed two years ago. He started on bosentan, but his exercise tolerance plateaued. After a thorough workup, his cardiologist added tadalafil and lowdose inhaled iloprost. Within six months, Alex could walk his dog for 30 minutes without breathlessnessa feat he hadnt managed in years. He credits the success to strict medication adherence, routine exercise, and open dialogue with his care team.
Expert Insight (Pulmonology Perspective)
Dr. Maya Patel, a pulmonologist at a leading academic center, notes: The most effective treatment plans are those built on current pulmonary hypertension treatment guidelines yet tailored to the individuals daily life. Were also watching sotatercept with optimism; it could become a cornerstone for patients who dont respond to existing drugs.
Patient Forum Highlights
On the Pulmonary Hypertension Associations forum, members frequently ask:
- Can I travel by plane? Answer: Yes, but bring supplemental oxygen if youre below 90% saturation.
- What symptoms signal worsening? Answer: Increasing shortness of breath, swelling in ankles, or fainting spells should prompt a doctor visit.
These real questions shape the practical advice you see throughout this article.
Helpful Resources
For deeper dives, consider these trusted sites:
- American Heart Association Pulmonary Hypertension Fact Sheets (search AHA pulmonary hypertension).
Conclusion
Theres no magic bullet, but there is a roadmap. Modern pulmonary hypertension treatment blends proven drugs, emerging science, surgical options, and lifestyle supportall balanced against each patients unique situation. By staying informed, partnering with a knowledgeable specialist, and embracing both medical and selfcare strategies, you can keep the pressure down and life moving forward.
If youve found a tip here that resonates, or you have a personal story to share, lets keep the conversation going. Reach out to a PHcenter, join a patient community, or simply ask your doctor about any of the therapies mentioned. You deserve care thats both cuttingedge and compassionate.
For related information on managing fluid and swelling that often accompany heart and lung conditions, see heart failure edema treatment which covers practical edema management strategies that can complement pulmonary hypertension care.
FAQs
What are the main medications used to treat pulmonary hypertension?
The primary medications include endothelin receptor antagonists (e.g., bosentan, ambrisentan), phosphodiesterase-5 inhibitors (e.g., sildenafil, tadalafil), soluble guanylate cyclase stimulators (riociguat), and prostacyclin analogues (e.g., epoprostenol, treprostinil). Calcium channel blockers may be effective for a select group of responders.
When is supplemental oxygen recommended for pulmonary hypertension patients?
Supplemental oxygen is used when blood oxygen levels fall below 90%, aiming to maintain 92-95% saturation to reduce heart strain and alleviate symptoms like fatigue.
Can pulmonary hypertension be cured with surgery?
For chronic thromboembolic pulmonary hypertension (CTEPH), pulmonary endarterectomy (PEA) is a potentially curative surgery with high success rates. However, it is a complex procedure suitable only for selected patients.
What new treatments for pulmonary hypertension are emerging?
Emerging therapies include sotatercept, which modifies disease pathways to reduce vascular remodeling, and low-dose imatinib targeting tyrosine kinase pathways. Both are promising but still under regulatory review.
How important are lifestyle changes in managing pulmonary hypertension?
Lifestyle adjustments such as low-impact exercise, low-sodium diet, and quitting smoking support medical therapy by improving heart function and overall health, but they do not replace prescribed treatments.