Targeted therapy lung cancer uses medicines that lock onto specific genetic changes inside tumor cells. If you or a loved one are facing stage 4 non-small cell lung cancer (NSCLC), those drugs can often slow the disease with fewer of the classic chemotherapy woesbut they also bring their own set of considerations. Below, I'll walk you through how it works, who can benefit, what's on the market right now, and how to balance the upside with the potential downsides. Think of this as a friendly chat over coffee, where I'm here to answer your questions and share a few stories I've heard along the way.
How It Works
What is targeted therapy for lung cancer?
In a nutshell, targeted therapy lung cancer drugs zero in on a molecular driver that fuels the tumor's growth. Instead of blasting all rapidly dividing cells like chemo does, these agents attach to a mutant protein or a specific pathwaythink of it as a lock and key. When the key fits, the lock can't turn, and the cancer cells stall.
How does it differ from chemotherapy and radiation?
| Aspect | Chemotherapy | Targeted Therapy |
|---|---|---|
| Mechanism | Damages any fast-growing cell | Blocks a specific mutant protein |
| Side effects | Hair loss, nausea, low blood counts | Rash, diarrhea, liver changes, occasional lung inflammation |
| Administration | IV every 23 weeks | Oral pill daily or IV infusion weekly |
| Typical Duration | 68 cycles | Until progression or intolerance |
The main takeaway? Targeted therapy often feels gentler on everyday life, but it's not free of risks.
Which molecular pathways are targetable?
The most common actionable pathways in NSCLC today include:
- EGFR (epidermal growth factor receptor)
- ALK (anaplastic lymphoma kinase)
- ROS1
- KRAS G12C
- BRAF V600E
- MET exon 14 skipping
- RET and NTRK fusions
Each has its own suite of drugs, and you'll hear terms like EGFR-targeted therapy lung cancer pop up a lot in discussions.
Why is genetic testing essential?
Before any pill is prescribed, doctors need to know which "lock" the tumor carries. Tissue biopsy is the gold standard, but a liquid biopsytesting circulating tumor DNA from a blood drawhas become a convenient alternative for many patients. Knowing the mutation not only opens the door to the right targeted drug, it also spares you from ineffective treatments.
Who Can Benefit
Is targeted therapy right for stage 4 NSCLC?
According to the 2025 NCCN guidelines, about 70% of patients with stage 4 NSCLC harbor a driver mutation that can be treated with a targeted agent. If your tumor tests positive for EGFR, ALK, KRAS G12C, or another target, you're likely a good candidate.
What are the most common actionable mutations?
Here's a quick prevalence snapshot in the United States:
- EGFR ~15%
- ALK ~5%
- ROS1 ~2%
- KRAS (overall) ~30% (with G12C making up ~13%)
- BRAF ~2%
These percentages vary by smoking history and ethnicity, but they give you a sense of how often a targetable mutation shows up.
Can patients without a known mutation use targeted drugs?
Generally, no. Using a targeted agent without the corresponding mutation is like trying to open a door with the wrong keyit won't work, and it can cause unnecessary toxicity. That said, some clinical trials explore off-label uses, but they're best pursued under a specialist's supervision.
How does an EGFR-targeted therapy differ from other TKIs?
| Drug | Target | Key Feature | Typical Dose |
|---|---|---|---|
| Erlotinib (Tarceva) | EGFR | First-generation TKI | 150mg PO daily |
| Osimertinib (Tagrisso) | EGFR T790M & sensitizing mutations | Third-generation, CNS-penetrant | 80mg PO daily |
| Afatinib (Gilotrif) | EGFR & HER2 | Irreversible binding | 40mg PO daily |
Osimertinib is often the go-to today because it reaches the brain and works against the common resistance mutation T790M.
Approved Drugs 2025
What targeted drugs are currently approved?
| Drug (Brand) | Target | FDA Approval Year | Formulation |
|---|---|---|---|
| Osimertinib (Tagrisso) | EGFR | 2015 (expanded 2020) | Oral capsule |
| Alectinib (Alecensa) | ALK | 2015 | Oral tablet |
| Lorlatinib (Lorbrena) | ALK/ROS1 | 2018 | Oral capsule |
| Sotorasib (Lumakras) | KRAS G12C | 2021 | Oral tablet |
| Adagrasib (Krazati) | KRAS G12C | 2025 | Oral tablet |
| Dabrafenib + Trametinib (Tafinlar + Mekinist) | BRAF V600E | 2017 | Oral tablets |
| Amivantamab-vmjw (Rybrevant) | EGFR & MET exon 14 | 2021 | IV infusion |
Notice the new pill for lung cancer that made headlines in early 2025? It's adagrasib, a KRAS G12C inhibitor that added another arrow to the targeted-therapy quiver.
What are the main side effects to expect?
While many patients tolerate these agents well, each class brings its own pattern:
- EGFR TKIs: Skin rash, diarrhea, and occasional low magnesium.
- ALK inhibitors: Fatigue, constipation, and rare liver enzyme elevations.
- KRAS G12C inhibitors: Nausea, vomiting, and modest elevations in liver enzymes.
- Combination regimens (e.g., EGFR TKI + anti-VEGF): Higher rates of hypertension and proteinuria.
If a serious problem like interstitial lung disease (ILD) pops up, the drug is stopped immediately.
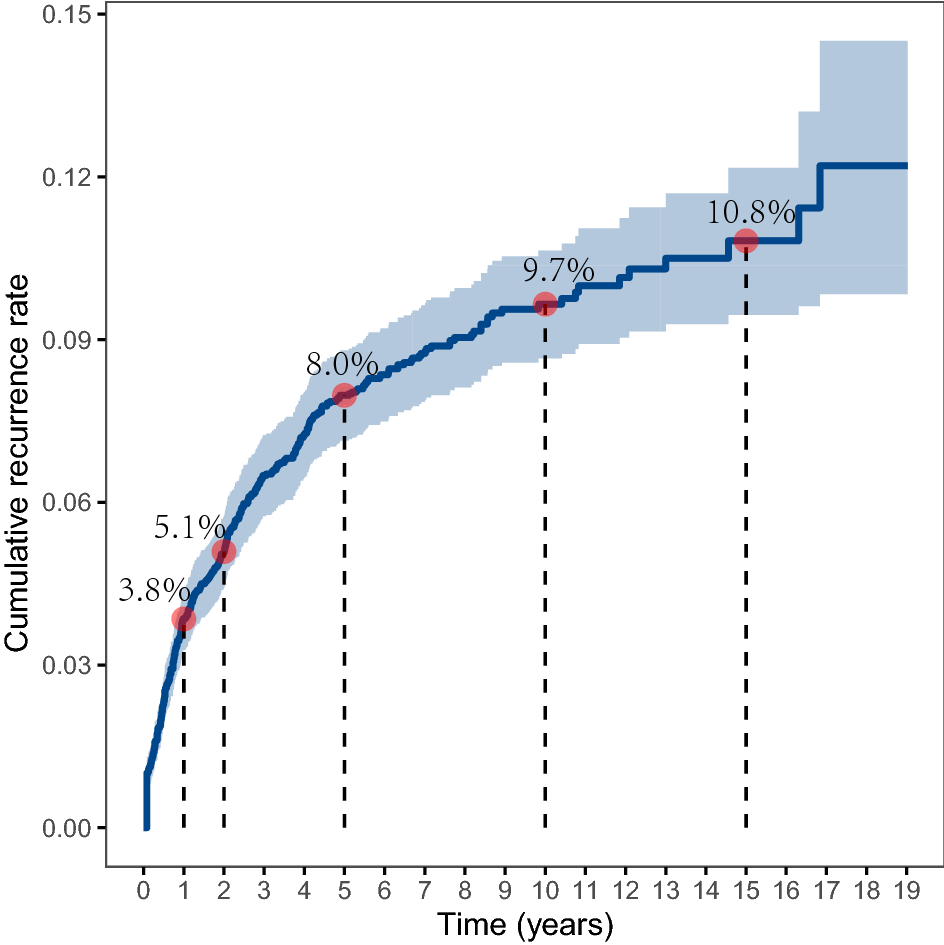
How do survival rates compare to chemo?
In landmark trials, patients on EGFR-targeted therapy lived a median of 1822 months versus about 12 months on platinum-based chemo. ALK inhibitors push median overall survival beyond 30 months in many series. KRAS G12C inhibitors are newer, but early data show a median OS of roughly 15 monthsstill an improvement over historical chemo for that subgroup.
For patients and families concerned about long-term survival with other cancers, it's helpful to look at broader cancer diet plan strategies and lifestyle adjustments that support overall health. This can be particularly relevant for those exploring prostate removal life expectancy, where outcomes are also shaped by treatment choices, patient health, and careful follow-up.
What is the new pill for lung cancer?
Adagrasib (brand name Krazati) received FDA approval in January 2025 for KRAS G12C-mutated NSCLC after progression on prior therapy. In the KRYSTAL-1 trial, the drug produced an overall response rate of 43% and a median progression-free survival of 6.5 months, offering hope to patients whose tumors carry this once "undruggable" mutation.
Benefits vs Risks
What are the survival benefits of targeted therapy?
Across the board, targeted therapy lung cancer improves both quantity and quality of life. For EGFR-mutated patients, 2-year survival now hovers around 55% versus roughly 30% with chemo alone. ALK-positive patients often exceed 70% 3-year survival when treated with second-generation inhibitors.
What side effects are unique to targeted therapy lung cancer?
Beyond the rash and diarrhea already mentioned, there are a few quirks:
- EGFR skin rash: Often called acne-like and can be managed with topical steroids.
- ILD (interstitial lung disease): Although rare (<5%), it can be life-threatening and requires immediate drug cessation.
- QT prolongation: Some TKIs affect heart rhythm, so baseline ECGs are recommended.
Most side effects are reversible once the dose is reduced or the medication is paused.
How does targeted therapy affect quality of life?
A study published in JCO Oncology Practice found that patients on oral TKIs reported higher scores on the EORTC QLQ-C30 questionnairemeaning less fatigue, better emotional functioning, and more ability to keep up with daily chores. One patient I spoke with described feeling normal enough to take her kids to the park again after weeks on osimertinib.
When should treatment be switched or stopped?
Doctors typically monitor disease with CT scans every 812 weeks. If imaging shows progression according to RECIST criteria, or if toxicity becomes unmanageable, the regimen is changed. Importantly, repeat biopsy (or liquid biopsy) at progression can uncover a new resistance mutation (e.g., EGFR T790M) that opens the door to a next-line targeted agent.
New Frontiers
What are the latest FDA approvals (20242025)?
Besides adagrasib, 2024 saw the approval of amivantamab-vmjw for EGFR exon 20 insertions and sotorasib's expanded indication for KRAS G12C after first-line therapy. These additions reflect a rapid pipeline that's reshaping treatment algorithms.
Can targeted therapy be combined with immunotherapy?
The idea is tempting: hit the tumor's driver mutation while also unleashing the immune system. Early trials like IMpower150 showed a survival boost when atezolizumab (an immunotherapy) was added to bevacizumab plus chemotherapy for EGFR-mutated patients. However, the combination of EGFR TKIs with PD-1/PD-L1 inhibitors can increase lung toxicity, so physicians often stagger the timing or choose carefully based on individual risk.
What clinical trials should patients consider?
ClinicalTrials.gov is the go-to for current studies. Look for Phase III KRAS G12C inhibitor or "Combination EGFR TKI + immune checkpoint inhibitor." Many trials now accept patients with stable brain metastases, which is a big plus for those dealing with CNS disease.
What does the future holdnext-gen pills?
Researchers are already testing KRAS G12D inhibitors (a mutation more common in smokers) and bispecific antibodies that can hit two targets at once. Antibody-drug conjugates (ADCs) that deliver a toxic payload directly to a mutant protein are also in early phases, promising a new wave of highly selective, potent treatments.
Quick FAQs
What is targeted therapy for lung cancer stage 4?
It's a class of drugs that blocks specific genetic drivers in advanced NSCLC, extending survival and often allowing patients to stay at home rather than spend weeks in a hospital.
How long can someone live on targeted therapy?
Median overall survival ranges from about 18 months for EGFR-mutated disease to over 30 months for ALK-positive cancers, though individual outcomes vary based on overall health, mutation type, and treatment adherence.
Are side effects reversible?
Most are. Rashes and diarrhea usually improve with dose adjustments or supportive meds. Serious events like ILD require stopping the drug, but once managed, patients can often switch to another targeted agent.
Do I need ongoing genetic testing?
Yes. Tumors can evolve. A liquid biopsy at progression often reveals new resistance mutations that dictate the next line of therapy.
Is targeted therapy covered by insurance?
In the United States, most major insurers cover FDA-approved targeted agents for the indicated mutation. Pharmaceutical companies also offer patient-assistance programs; a quick call to the drug's support line can clarify eligibility.
Talk to Your Doctor
Preparing for your oncology appointment can make the whole process feel less overwhelming. Here's a quick checklist you can print out:
- Bring a copy of your most recent pathology report.
- Write down every medication, supplement, and over-the-counter product you're taking.
- Ask: Which driver mutations does my tumor have, and what targeted options are available?
- Inquire about clinical trial eligibilitymany centers have lists you can review on the spot.
- Discuss financial assistance: Do you have information on copay help or manufacturer programs?
- Request a written treatment plan that includes medication schedule, monitoring labs, and imaging timeline.
Having these questions ready shows you're engaged and helps the clinician tailor the conversation to what matters most to you.
Trusted Resources
For deeper dives, these organizations keep their guidelines up-to-date and are widely respected:
- National Cancer Institute
- Peer-reviewed journals such as Journal of Clinical Oncology and Lung Cancer for the latest trial data.
Sticking to reputable sources ensures you're getting evidence-based information rather than hype.
Conclusion
Targeted therapy lung cancer has reshaped the outlook for many people facing stage 4 disease. By matching a drug to a specific genetic driver, we can often extend survival, improve quality of life, and keep daily routines more normal. Yet the journey isn't without challengesside effects, resistance, and the need for ongoing testing mean that vigilance and open communication with your care team are essential. If you're navigating a new diagnosis or weighing treatment choices, use the checklist above, explore the trusted resources, and consider talking to a clinical-trial nurse. You deserve clear, compassionate information, and the right targeted therapy could be a pivotal piece of your story.
What's your experience with targeted therapy? Share your thoughts in the comments, or reach out if you have questions. We're all in this together.
FAQs
What is targeted therapy lung cancer?
Targeted therapy lung cancer uses drugs that block specific genetic mutations or pathways that drive tumor growth, allowing treatment to focus on cancer cells while sparing most normal tissue.
How do I know if I’m eligible for targeted therapy?
Eligibility is determined by molecular testing of the tumor (tissue or liquid biopsy). If a driver mutation such as EGFR, ALK, KRAS G12C, or others is found, a matching targeted agent can be prescribed.
What are the common side‑effects of targeted therapy lung cancer?
Side‑effects vary by drug class but often include skin rash, diarrhea, liver‑enzyme elevations, fatigue, and, rarely, interstitial lung disease (ILD). Most are manageable with dose adjustments or supportive care.
How often should I get genetic testing while on targeted therapy?
Baseline testing is done before starting treatment. At disease progression (usually confirmed by scans every 8‑12 weeks), a repeat biopsy or liquid biopsy is recommended to identify resistance mutations that guide the next line of therapy.
Can targeted therapy be combined with immunotherapy?
Combination is an active research area. Some regimens show benefit, but certain EGFR or ALK inhibitors plus PD‑1/PD‑L1 blockers can increase lung toxicity, so combinations are selected carefully and often staggered.