Looking for a quick answer? A suprapubic prostatectomy is an open surgery where the surgeon makes a lowmidline abdominal cutusually just below the belly buttonto remove part or all of an enlarged prostate. Its often the goto option when the gland is really big (think80g or more) or when lessinvasive techniques just wont do the job.
Why does this matter to you? Because the right surgical choice can mean quick relief from painful urinary symptoms, while the wrong one can bring unnecessary hassle. Below, I walk you through everything you need to knowbenefits, risks, what the operation looks like, and how to prepareso you can feel confident making an informed decision.
Overview
Suprapubic vs. Retropubic
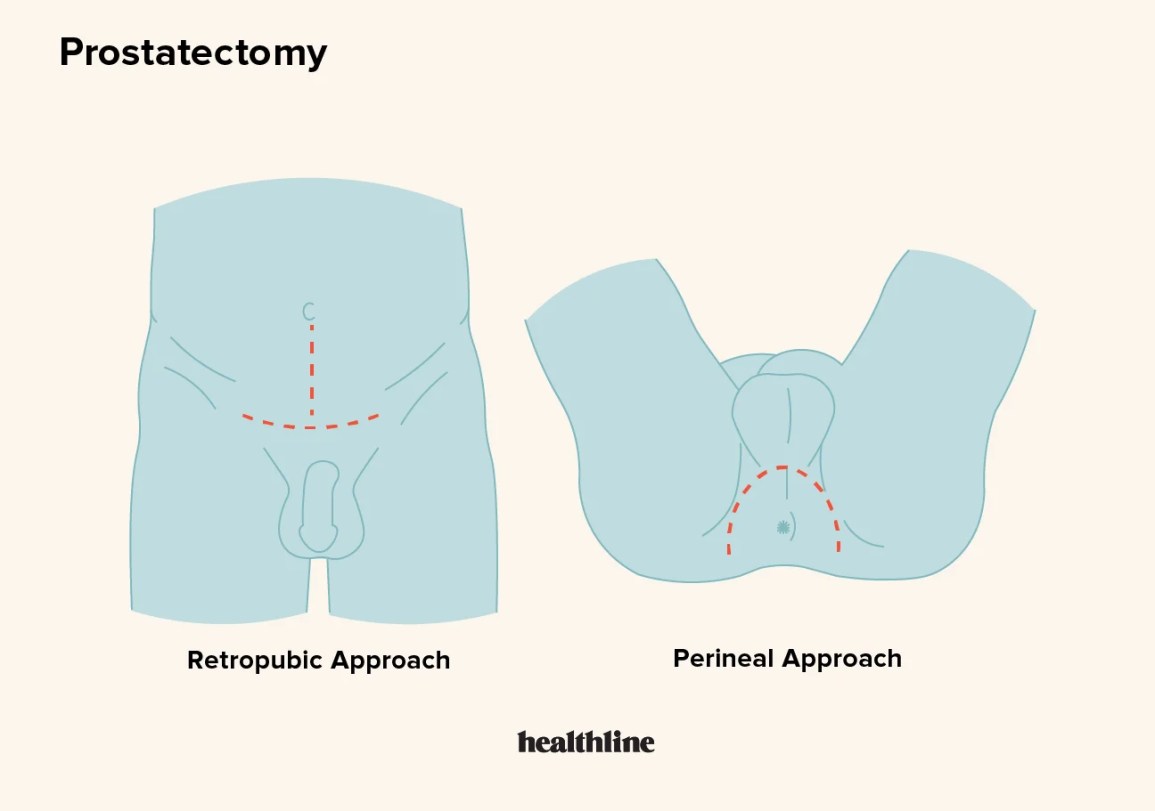
Both approaches aim to remove the prostate, but they get there through different doors. The suprapubic (or transvesical) route goes through the bladder, accessed via a small abdominal incision. The retropubic (often called Millins prostatectomy) approaches the gland from behind the pubic bone, staying outside the bladder. In practice, the choice hinges on prostate size, surgeon experience, and any prior procedures youve had.
When Its Recommended
Most urologists reserve the suprapubic technique for prostates larger than 80g, for patients who have already tried medications or laser therapies without success, or when anatomy makes the transurethral route too risky. If youve been told your prostate is giant and youre stuck with frequent nighttime trips to the bathroom, this might be the surgery that finally gives you relief. If you're preparing for surgery, reviewing prostatectomy recovery expectations can help set realistic timelines for catheter removal and return to activity.
Who Performs It
Only boardcertified urologists who have completed a fellowship in urooncology or reconstructive urology should be doing this operation. Look for surgeons who log at least 50 suprapubic or retropubic cases a yearhigher volumes translate to lower complication rates, according to several peerreviewed studies.
Comparison Table
| Feature | Suprapubic | Retropubic (Millin) | Perineal | Transurethral (TURP) |
|---|---|---|---|---|
| Incision | Lowmidline abdomen | Lower abdomen, retropubic space | Perineal groove | No external incision |
| Ideal size | >80g | 3080g | 3070g | <80g |
| Hospital stay | 24days | 24days | 23days | Outpatient |
| Blood loss | Moderatehigh | Moderate | Lowmoderate | Low |
| Typical complications | Bleeding, infection, incontinence | Similar | Wound issues | Erectile dysfunction, retrograde ejaculation |
StepbyStep
Preop Prep
Before you step into the OR, youll likely have a full set of labsPSA, CBC, renal panelplus imaging (ultrasound or MRI) to map out the gland. Most surgeons prefer general anesthesia, but spinal can be an option for some patients. Youll also get a bowel prep and a checklist of meds to hold (think blood thinners) to keep bleeding under control.
Operative Steps
- Positioning: Youll lie on your back, with the table break under the belly buttonthis gives the surgeon a clear view of the lower abdomen.
- Incision: A 610cm cut is made either in the midline or as a Pfannenstiel (the bikini line) incision. This is the youll see in most surgical videos.
- Bladder entry: The surgeon opens the bladder (a transverse cystotomy) and slides a Foley catheter in to keep the bladder drained.
- Enucleation: Using blunt dissection, the adenoma (the enlarged part) is carefully peeled away from the capsule, much like removing a seed from a fruit.
- Hemostasis & closure: Electrocautery stops bleeding, then the bladder wall is sutured with absorbable stitches. A suprapubic catheter is left in place for about a week.
- Skin closure: The skin is usually closed with subcuticular sutures or skin glue for a neat scar.
Postop Care
After surgery, youll be monitored in a recovery room for vitals and urine output. Pain management typically involves a mix of NSAIDs and shortacting opioids. The catheter stays for 57days, giving the bladder a chance to heal before you start emptying on your own. Early ambulation (getting out of bed within 24hours) and a gradual return to solid foods help keep complications low.
Benefits
Symptom Relief
Most men notice a dramatic drop in urinary frequency, urgency, and weak stream within weeks. Objective studies show a 7080% increase in maximum flow rate (Qmax) after a successful suprapubic prostatectomy.
When It Outshines Alternatives
If your prostate is giant (over 100g), laser or TURP would require multiple separate resections, lengthening the hospital stay and raising infection risk. The open suprapubic route lets the surgeon remove the whole gland in one go, sparing you from staged procedures.
PatientCentred Advantages
- Singlestage removalno need for followup surgeries.
- Direct visual inspection of the bladder, allowing the surgeon to spot any hidden tumors.
- Quick return to normal daily activities for most patients once the catheter is out.
Risks & Complications
Common Intraoperative Risks
Even with an experienced surgeon, youre looking at an average blood loss of 5001000ml. About 510% of patients need a transfusion. Rarely, the ureters or bladder neck can be injured, which would require additional repair.
Postoperative Complications
| Complication | Frequency | Management Tips |
|---|---|---|
| Urinary incontinence (stress/urge) | 1015% | Pelvic floor rehab, anticholinergics |
| Bladder neck contracture | 35% | Endoscopic dilation |
| Infection / sepsis | 24% | Prophylactic antibiotics, wound care |
| Erectile dysfunction | 510% | Counselling, PDE5 inhibitors |
| Suprapubic catheter issues | 5% | Proper catheter care, early removal |
LongTerm Considerations
Some men later need a sling or artificial urinary sphincter to manage lingering incontinence. A small percentage may also develop a need for secondary procedures, such as dilation of a scarred bladder neck. Knowing these possibilities up front helps you weigh the overall picture.
Minimising Risk
Choose a surgeon with a high case volume, request intraoperative ultrasound to protect the ureters, and follow a strict postop mobilization and DVTprophylaxis plan. These steps have been shown to shave off a few percent from complication rates, according to a 2023 urology outcomes review.
FAQs
Is suprapubic the same as retropubic?
No. Suprapubic (transvesical) goes through the bladder via an abdominal cut, while retropubic (Millins) works behind the pubic bone without entering the bladder. The two differ in incision site, ideal prostate size, and some sideeffect profiles.
How long is the incision?
Typically 610cm, though the exact length depends on your body habitus and the size of the gland being removed.
Can I go home the same day?
Usually not. Most hospitals keep you for 24days to monitor for bleeding, ensure the catheter works, and start early mobilization.
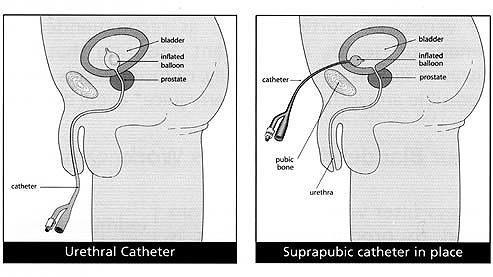
What is a suprapubic catheter?
Its a tube that exits through the same lowmidline incision you made for the surgery, allowing the bladder to drain while it heals. Its usually removed after a week, once the bladder wall has sealed.
What alternatives exist for a large prostate?
Besides suprapubic prostatectomy, options include roboticassisted laparoscopic simple suprapubic prostatectomy (RALSSP), Holmium laser enucleation (HoLEP), and open retropubic prostatectomy. Each has its own pros and constalk to your urologist to find the best fit.
RealWorld Perspectives
Patient Story
John, 68, was waking up three times a night to pee and was terrified of falling. His prostate measured 120g, and medications didnt help. After a suprapubic prostatectomy, he reports a smooth stream and only one bathroom trip before bedtime. At threemonth followup, his PSA dropped to normal levels and hes back to gardening without a single nighttime interruption.
Surgeon Insight
Dr. Elena Ramirez, a boardcertified urologist at a major academic center, says, When the prostate is truly massive, the suprapubic route gives us the visibility and control we need. Its not the first line, but for the right patient its a gamechanger. She emphasizes that surgeon experience and a clear discussion of risks are essential for a successful outcome.
Guidelines & Standards
The American Urological Association (AUA) includes suprapubic prostatectomy in its algorithm for managing large prostates that are refractory to medical therapy. Following these guidelines helps ensure you receive care that aligns with the latest evidence.
Preparation Checklist
Before Surgery
- Complete all labs and imaging (PSA, MRI, CBC).
- Stop blood thinners as instructed (usually 57days prior).
- Arrange for a caregiver to stay with you the first night.
- Clear out your bathroom for easy access (nightlight, grab bars).
- Pack a small bag with comfortable clothing, personal hygiene items, and any prescribed medications.
What to Ask Your Surgeon
- How many suprapubic prostatectomies have you performed in the past year?
- What is the expected hospital stay and pain management plan?
- What are the specific risks for someone with my health profile?
- When can I expect the catheter to be removed?
- What followup schedule should I anticipate?
Conclusion
A suprapubic prostatectomy is a safe, wellestablished option for men with very large prostates or when newer, lessinvasive techniques arent viable. The procedure can deliver rapid, lasting relief from urinary symptoms, but it does come with a clear set of risks that need to be weighed carefully. By choosing an experienced surgeon, preparing thoroughly, and staying informed about both benefits and possible complications, you can make a confident decision that aligns with your health goals.
If youre facing this choice, schedule a candid conversation with a qualified urologist. Ask the questions that matter to you, bring a trusted friend or family member to the appointment, and remember that you deserve a treatment plan that respects both your body and your peace of mind.
FAQs
What is a suprapubic prostatectomy?
A suprapubic prostatectomy is an open surgery involving a low midline abdominal incision through the bladder to remove part or all of an enlarged prostate, typically used for prostates larger than 80 grams.
When is suprapubic prostatectomy recommended?
It is recommended for very large prostate glands (over 80g), when medications or less invasive treatments have failed, or anatomical factors make other surgical approaches risky.
How long is the hospital stay after the procedure?
The typical hospital stay ranges from 2 to 4 days to monitor for bleeding, ensure catheter functionality, and start recovery.
What are the main risks and complications of this surgery?
Common risks include moderate to high blood loss, urinary incontinence, bladder neck contracture, infection, erectile dysfunction, and issues with the suprapubic catheter.
What should I expect during recovery?
You will have a suprapubic catheter for about a week, with pain managed through NSAIDs and opioids. Most patients experience significant relief of urinary symptoms and can resume normal activities gradually after catheter removal.