Hey there! If youve ever heard the term subclinical hypothyroidism and felt a wave of confusion, youre not alone. In short, its a mild thyroid imbalance where your TSH (thyroidstimulating hormone) is a little high, but your thyroid hormones (T4/T3) are still in the normal range. It can feel like a silent issueyour labs raise a flag, yet you might not notice any dramatic symptoms. The big question most of us face is: should I treat it, or can I just watch and wait? Lets unpack everything you need to know, from what it really means to how to manage it in everyday life.
What Is Subclinical Hypothyroidism?
Understanding the subclinical label
Subclinical simply means below the clinical threshold. In thyroid health, it indicates that the hormone levels that tell the thyroids story (free T4 and free T3) are still normal, but the pituitary gland is asking for more thyroid output, so TSH rises. Think of TSH as the thermostat; when it notices the room getting a little chilly, it turns up the heat. In this case, the thermostat (TSH) is nudging the thyroid to work a bit harder, even though the room temperature (T4/T3) seems fine.
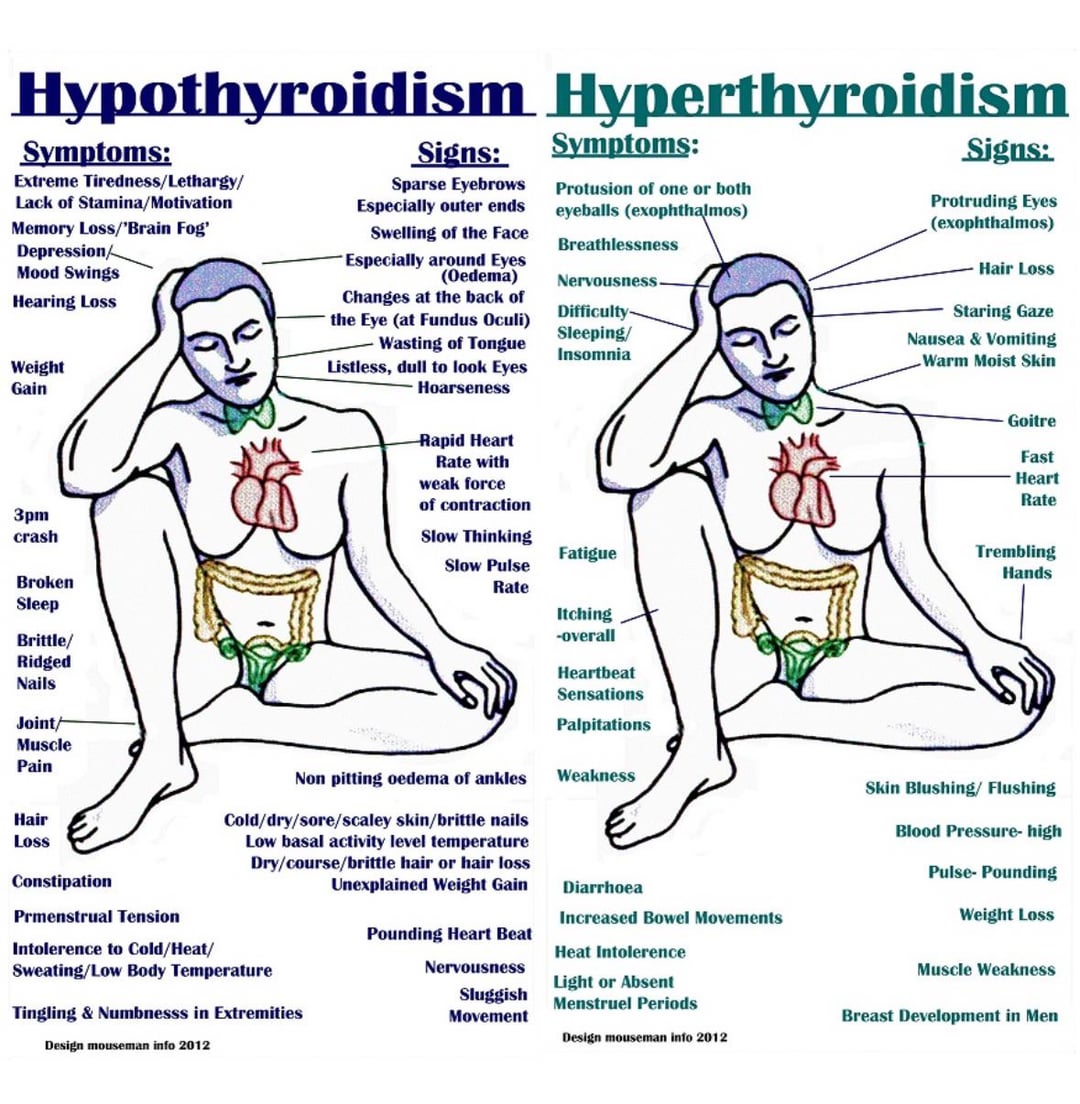
How it differs from overt hypothyroidism
When overt hypothyroidism kicks in, both TSH is high and T4/T3 drop below normal. Thats when classic symptomspronounced fatigue, weight gain, dry skinbecome unmistakable. Subclinical hypothyroidism sits in that gray zone: labs whisper a concern, but you might feel off in subtle ways.
Quick visual guide
Below is a simple diagram (feel free to sketch it on a napkin) that shows where subclinical hypothyroidism lands on the TSHT4 spectrum.
| Condition | TSH | Free T4 |
|---|---|---|
| Normal | 0.44.0mIU/L | Within reference range |
| Subclinical hypothyroidism | >4.0mIU/L (often 410) | Normal |
| Overt hypothyroidism | >10mIU/L | Low |
Who Is Most Affected?
Risk groups you might recognize
Women are about five to eight times more likely to develop this condition than menhormones, anyone? Age is another factor; prevalence climbs after 60. Autoimmune diseases, especially Hashimotos thyroiditis, are the biggest culprits, and certain medications (like lithium or amiodarone) can tip the scales.
Subclinical hypothyroidism in pregnancy
Pregnant folks need a special shoutout. Even a modest TSH rise can affect fetal brain development. Studies show that treating pregnant women with subclinical hypothyroidism can lower the risk of preterm birth and improve newborn IQ scores. If youre planning a family or already expecting, flag this on your checklist.
Realworld story
Anna, a 32yearold teacher, discovered she had a TSH of 6.2mIU/L during her first prenatal visit. She felt a bit more tired than usual but chalked it up to morning sickness. Her obstetrician, aware of the guidelines, started a low dose of levothyroxine. By her third trimester, her energy bounced back and her babys growth chart stayed on track.
Typical Subclinical Symptoms
What you might actually feel
Because hormone levels are still within range, symptoms can be subtle. Common complaints include:
- Persistent lowgrade fatigue (that just cant shake feeling)
- Cold intolerancereaching for an extra sweater for no reason
- Mild weight gain or difficulty losing weight
- Brain fog or trouble concentrating
- Dry skin or hair that feels a little brittle
Symptoms in females specifically
Women may notice menstrual irregularitieslighter or heavier periods, or a shift in cycle length. Some also report a slight increase in cholesterol levels, which can be a silent warning sign.
Quick comparison
| Feature | Subclinical | Overt |
|---|---|---|
| TSH level | 410mIU/L | >10mIU/L |
| Free T4/T3 | Normal | Low |
| Fatigue | Mildmoderate | Severe |
| Weight change | Small gain | Noticeable gain |
| Cholesterol | May rise | Often high |
Main Causes and Risks
Autoimmune thyroiditis (Hashimotos)
The most common driver is the bodys own immune system attacking thyroid tissue, causing inflammation and a gradual decline in function. Even before the gland falters, the pituitary senses the strain and nudges TSH upward.
Iodinetoo little or too much
Iodine is essential for thyroid hormone production. In some regions, deficiency still lurks; in others, excess from supplements can paradoxically suppress thyroid activity and then rebound. Balance is key.
Medications and other conditions
Drugs like lithium, interferon, or amiodarone can interfere with thyroid hormone synthesis. Pituitary tumors or rare genetic disorders also have a role, though theyre less common.
ICD10 coding note
If you or your clinician need to log this in medical records, the standard code is E03.9 (unspecified hypothyroidism). Having the right code helps insurance and ensures you get appropriate followup.
How Doctors Diagnose It
Lab thresholds you should know
Most guidelines define subclinical hypothyroidism as a TSH above 4.0mIU/L (sometimes the cutoff is 4.5) with a normal free T4. Some labs use slightly different ranges, so its wise to ask your provider what their reference values are.
Why repeat testing matters
TSH can wobble due to acute illness, stress, or even time of day. Doctors usually recommend a repeat test in 36 months to see if the elevation persists or worsens. Consistent trends are far more telling than a single spike.
Additional tests for a fuller picture
- Antithyroid peroxidase (TPO) antibodies high levels suggest Hashimotos.
- Lipid panel thyroid dysfunction can raise LDL cholesterol.
- Pregnancyspecific tests free T4, especially in the first trimester.
When Treatment Is Needed
Guideline thresholds
According to the , treatment is usually recommended if:
- TSH persists above 10mIU/L.
- Youre pregnant, planning pregnancy, or have a history of miscarriage.
- Theres evidence of heart disease, high cholesterol, or a rapid rise in TSH.
- Youre under 65 and experience clear symptoms that affect quality of life.
Balancing benefits and risks
Levothyroxine is safe for most people, but overtreatment can lead to anxiety, palpitations, or bone loss. Thats why many clinicians start with a low dose (e.g., 25g) and titrate based on repeat labs. The goal isnt to fix a number but to bring you back to feeling normal.
Treatment Options Explained
Levothyroxine the gold standard
This synthetic T4 replacement mimics the hormone your thyroid would normally make. Most patients take it once daily, preferably on an empty stomach, and wait at least 30 minutes before breakfast or coffee.
Lifestyle and diet tweaks
While medication does the heavy lifting, supportive habits can smooth the journey:
- Iodine intake aim for 150g/day (iodized salt, dairy, fish).
- Selenium Brazil nuts, sunflower seeds, or a modest supplement can help the thyroid convert T4 to the active T3.
- Limit excessive soy and cruciferous veggies raw, as they contain goitrogens that may hinder hormone synthesiscooking usually neutralizes them.
- Regular aerobic exercise can boost metabolism and improve cholesterol levels.
Sample subclinical hypothyroidism diet
| Meal | Key Foods | Why It Helps |
|---|---|---|
| Breakfast | Greek yogurt, berries, a handful of Brazil nuts | Protein, antioxidants, selenium boost |
| Lunch | Grilled salmon, quinoa, steamed spinach | Omega3s & iodine, iron, minimal goitrogens |
| Dinner | Turkey stirfry with bell peppers, cooked broccoli, brown rice | Lean protein, cooked veggies reduce goitrogenic effect |
| Snack | Wholegrain toast with avocado | Healthy fats, Bvitamins for energy |
Managing the Condition LongTerm
Monitoring schedule
After starting treatment or deciding to watch, most doctors suggest checking TSH every 612 months. If youre on medication, the first followup is often at 6 weeks to see how your dose is settling.
When to adjust or reconsider therapy
Signs that your dose may need tweaking include new onset tremor, heart palpitations, insomnia, or unexpected weight loss. Conversely, if you feel consistently sluggish despite medication, a dose increase might be warranted.
Tools to keep you on track
Consider downloading a simple thyroidtracking sheet (you can create one in Excel). Log your TSH results, medication dose, symptoms, and any lifestyle changes. Spotting patterns over months is surprisingly empowering.
Trusted Resources & References
Where to find reliable information
We all love a quick answer, but the best decisions come from credible sources. Here are a few you can rely on:
- Cleveland Clinic clear explanations of thyroid labs and treatment pathways.
- American Thyroid Association uptodate guidelines for clinicians and patients.
- National Institutes of Health (NIH) deep dives into thyroid physiology and research studies.
Keep these sites bookmarked; theyre gold mines when you have a new question or need to doublecheck something you heard at the doctors office.
Conclusion
Subclinical hypothyroidism can feel like an invisible hurdleyour labs are flashing a caution sign, but you might not notice anything dramatically wrong. The good news? With the right balance of monitoring, lifestyle tweaks, and, when needed, gentle medication, most people can keep their thyroid humming along happily. If youve had a recent test that showed a high TSH, take a deep breath, chat with your healthcare provider, and consider the steps weve outlined here. You deserve clear answers and a plan that feels both safe and effective.
Whats your experience with thyroid testing? Have you tried any of the diet suggestions or felt a difference after treatment? Share your thoughts, and lets keep the conversation going.
For readers exploring related thyroid treatment choices, many find comparing options helpful for example, learning about Armour vs levothyroxine can clarify differences between dessicated thyroid and synthetic T4 therapy.
FAQs
What is subclinical hypothyroidism?
Subclinical hypothyroidism is a mild thyroid disorder where TSH (thyroid-stimulating hormone) is elevated above normal but thyroid hormones T4 and T3 remain within the normal range. It often causes subtle or no symptoms.
Who is most at risk for subclinical hypothyroidism?
Women, especially over age 60, people with autoimmune thyroid diseases such as Hashimoto's thyroiditis, and those taking certain medications like lithium are most at risk. Pregnant women also require careful monitoring due to fetal risk.
What symptoms might indicate subclinical hypothyroidism?
Symptoms are often subtle and can include mild fatigue, cold intolerance, slight weight gain, brain fog, dry skin, and menstrual irregularities in women.
When should subclinical hypothyroidism be treated?
Treatment is generally recommended if TSH is consistently above 10 mIU/L, if symptoms affect quality of life, if the patient is pregnant or planning pregnancy, or if there is evidence of heart disease or elevated cholesterol.
What is the standard treatment for subclinical hypothyroidism?
Levothyroxine, a synthetic thyroid hormone (T4), is the gold standard treatment. It is usually started at a low dose and adjusted based on symptoms and lab results. Lifestyle and diet adjustments can support thyroid health.