Lets cut to the chase: spinal injections can bring rapid pain relief, but they also come with a handful of shortterm annoyances and a few rare, serious complications. If youre weighing whether to say yes to an epidural steroid shot, you deserve the straighttalkno fluff, no jargon, just the facts you need to make a confident decision.
In this post well walk through why doctors recommend these injections, what you might feel during and after the procedure, the dark side that many patients only hear whispers about, and practical steps you can take to keep yourself as safe as possible. Think of me as that knowledgeable friend whos been through a few injections and has talked to specialistshere to help you navigate the maze of spinal injection risks.
Why Choose Spinal Injections
What conditions are they used for?
Spinal (epidural) steroid injections are most commonly offered for:
- Herniated discs causing sciatica
- Spinal stenosis that squeezes nerves
- Facet joint arthritis
- Postsurgical pain or failed back surgery syndrome
Whats the expected benefit?
Most patients experience a 3070% reduction in pain that can last from a few weeks up to six months. The boost in mobility often lets them finally start physical therapy or return to daily chores theyd been avoiding.
Table: Typical Indications vs. Alternative Therapies
| Condition | Spinal Injection | Alternative Options |
|---|---|---|
| Chronic sciatica | Epidural steroid injection | Physical therapy, oral NSAIDs, nerveblock meds |
| Spinal stenosis | Facet joint injection | Decompression surgery, activity modification |
| Postsurgery pain | Caudal epidural injection | Rerehab program, acupuncture |
Types & Levels Explained
Where do doctors inject?
Injections are targeted to specific vertebral levels. The most common spots are:
- L4L5 lumbar epidural steroid injection directly addresses lowerback and leg pain.
- L5 epidural steroid injection side effects often used when the pain radiates down the thigh into the calf.
- Cervical, thoracic, facet, or sacroiliac injections for neck or upperback issues.
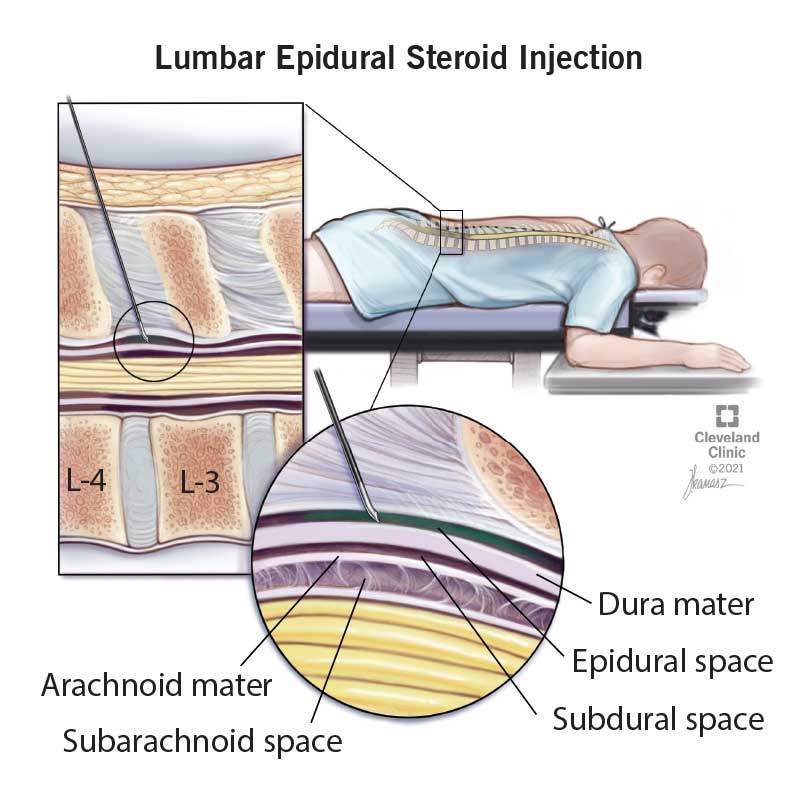
How painful is a lumbar epidural steroid injection?
Most patients describe a brief pressure or sting that feels like a quick pinprick. Real pain is usually under a 5/10 on the scale and fades within a few minutes once the needle is removed. A little discomfort is normal, but anything that feels like sharp, burning after the procedure warrants a call to your doctor.
Stepbystep: What youll feel
- Lie facedown on a padded table.
- Local anesthetic numbs the skinyou might feel a cool tingling.
- The doctor guides the needle with fluoroscopy (realtime Xray) or ultrasound.
- Youll sense a push as the medication is injected.
- After the needles out, youll stay for a short observation period (usually 1530 minutes).
Common Mild Side Effects
Immediate reactions
Its normal to have a little soreness at the injection site, a brief headache, or mild nausea. These symptoms usually settle within a day or two.
Shortterm neurological signs
Some patients notice temporary numbness, tingling, or even brief leg weakness after an epidural steroid injection. In most cases the feeling fades in a few hours. If weakness persists beyond 24hours, call your provider right away.
Frequency snapshot (according to the )
- Injectionsite pain: ~0.33%
- Transient headache: 12%
- Temporary leg weakness: ~0.14%
Rare Serious Complications
Infection & sepsis
Even with sterile technique, a small number of patients develop an infection that can spread to the spinal canal. Symptoms include fever, worsening pain, or drainage from the injection site.
Bleeding or hematoma
If youre on blood thinners, a bleed can accumulate around the spine, potentially compressing nerves. That\'s why a thorough medication review is mandatory before the procedure.
Nerve damage or permanent weakness
Although extremely rare, a needle misplacement can injure a nerve root, leading to lasting weakness or even paralysis. The has issued warnings about this risk and recommends limiting the number of injections per year.
Dural puncture & CSF leak
A wet tap can happen when the needle punctures the dura the protective membrane around the spinal cord. This may cause a postdural puncture headache that feels worse when you sit up.
Cardiovascular, vision loss, stroke, or death
These catastrophic events are exceedingly uncommon (<0.01% incidence) but have been documented in large case series. They underline the importance of a skilled injector and proper patient selection.
Comparison: Mild vs. Rare vs. Very Rare Risks
| Risk Category | Typical Incidence | Typical Outcome |
|---|---|---|
| Mild (soreness, headache) | 15% | Selflimited, resolves in days |
| Rare (infection, bleeding) | 0.10.5% | Treated with antibiotics or observation |
| Very Rare (nerve injury, stroke) | <0.01% | May need surgery or intensive care |
LongTerm Risks Overview
How do longterm side effects show up?
Repeated steroid exposure can affect your body beyond the spine. Potential longterm issues include:
- Adrenal suppression the bodys natural cortisol production may dip.
- Bone density loss chronic steroids can hasten osteoporosis.
- Elevated blood sugar especially concerning for diabetics.
The truth about epidural steroid injections
A 2023 systematic review in Spine concluded that while shortterm pain relief is welldocumented, the evidence for lasting functional improvement after multiple injections is mixed. In other words, theyre great for a reset but not a permanent fix.
Key study snapshots
- Smith et al., 2022 1,245 patients, 48% reported >50% pain relief at 3months.
- Lee & Patel, 2023 Found a 0.8% rate of persistent hyperglycemia in diabetic patients after 4+ injections.
Assessing Your Personal Risk
Which health factors raise your odds?
Consider these red flags before signing up:
- Uncontrolled diabetes or highbloodsugar levels.
- Use of anticoagulants (warfarin, aspirin, DOACs).
- Previous spinal surgery or scar tissue at the injection level.
- Active infection anywhere in the body.
How many injections is too many?
Guidelines from the American Academy of Orthopaedic Surgeons (AAOS) suggest limiting epidural steroids to no more than three injections per year, spaced at least 68 weeks apart. The goal is to avoid cumulative steroid load while still offering relief.
When to say No redflag symptoms
If you notice any of these after a shot, call your clinician immediately:
- Severe, worsening pain rather than improvement.
- Fever or chills.
- New or increasing weakness in the legs.
- Sudden vision changes or loss of bladder control.
Preprocedure checklist (what to ask your doctor)
- What imaging guidance will you usefluoroscopy or ultrasound?
- How many injections have you performed at this level?
- What is the exact medication and dose you plan to inject?
- What postprocedure signs should I watch for?
- Can we schedule a followup to assess effectiveness?
Strategies to Minimize Risks
Choose an experienced injector
Evidence shows that clinicians who have performed >100 spinal injections have significantly lower complication rates. Dont be shyask about their volume of cases.
Imaging guidance matters
Fluoroscopy provides realtime Xray confirmation of needle placement, while ultrasound avoids radiation and can be just as accurate in skilled hands. Studies suggest that imaging reduces blindneedle mishaps by up to 70%.
Postprocedure care tips
- Stay upright for at least 30 minutes; avoid lying flat for the first hour.
- Hydrate wellfluids help flush any residual medication.
- Monitor the injection site for swelling, redness, or drainage.
- Resume gentle activity (e.g., short walks) as tolerated; avoid heavy lifting for 2448hours.
Infographic idea (for later): DayofInjection Timeline
RealWorld Stories & Cases
Case A: Quick relief with minimal side effects
Mike, 45, suffered from chronic lowerback pain due to a L4L5 disc bulge. After a single L4L5 lumbar epidural steroid injection, his pain dropped from an 8/10 to a 2/10 within two days. He reported mild soreness for 24hours but was able to start a supervised PT program within a week.
Case B: Leg weakness that prompted fast action
Linda, 62, received an L5 epidural steroid injection for sciatica. Six hours later she noticed her left foot felt floaty. Recognizing the warning sign, she called her clinic. An urgent MRI ruled out a hematoma, and the physician prescribed a short course of steroids to reduce inflammation. Within three days the weakness resolved completely.
Quote from Dr. Elena Ramirez, MD Pain Medicine Specialist
Every injection is a riskvsbenefit conversation. The key is honesty about possible outcomes and vigilant followup. When patients understand the numberslike a 0.14% chance of temporary leg weaknessthey can make truly informed choices.
Summing It All Up
Spinal injection risks exist on a spectrum. Most people experience only mild, shortlived discomfort and enjoy solid pain relief. A very small subset may face serious, even lifechanging complications, which is why choosing a skilled provider, asking the right questions, and staying alert after the procedure are nonnegotiable.
Remember, the goal isnt to scare youits to empower you. Armed with the right knowledge, you can weigh the benefits against the risks, discuss realistic expectations with your doctor, and take proactive steps to stay safe.
If you found this guide helpful, why not grab the free Spinal Injection RiskAssessment Checklist linked below? And feel free to share your own experiences in the commentsyour story could be the exact thing someone else needs to hear.
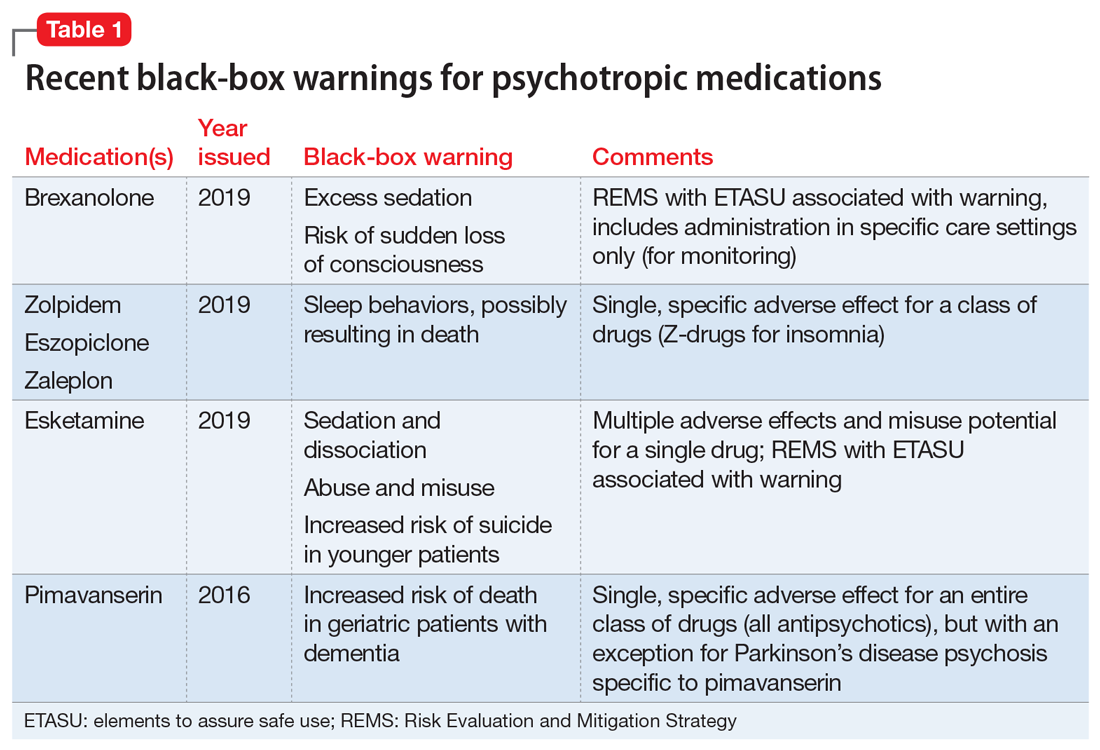
For related medication safety information, see the article on drug safety warnings which offers practical tips on recognizing serious drug side effects that could interact with steroids or other medications you may be taking.
FAQs
What are the most common mild side effects after a spinal injection?
Most patients experience brief soreness at the injection site, a mild headache, or temporary tingling that usually resolves within a couple of days.
How many spinal injections are considered safe in a year?
Guidelines recommend no more than three epidural steroid injections per year, spaced at least 6–8 weeks apart, to limit cumulative steroid exposure.
What signs indicate a possible infection after the procedure?
Fever, worsening pain, redness, swelling, or drainage from the injection site are warning signs that should prompt an immediate call to your doctor.
What questions should I ask my doctor before the injection?
Ask about the imaging guidance used, the provider’s experience with the specific injection level, the medication and dose planned, post‑procedure warning signs, and the schedule for follow‑up evaluation.
Are there alternatives to spinal injections for back pain?
Yes—options include physical therapy, oral NSAIDs, nerve‑block medications, activity modification, and, in select cases, surgical decompression or minimally invasive procedures.