Ever woken up to a lone, high-pitched ring that seems to live only in one ear? It's unnerving, right? The good news is that most of the time this one ear tinnitus isn't a mystery at allit's a signal that something in the ear or nearby needs attention, and there are clear steps you can take.
Below we'll walk through why unilateral tinnitus happens, when you should get it checked, and the range of treatments that actually work. Think of this as a friendly chat over coffee, with a dash of science to keep things reliable.
Understanding Unilateral Tinnitus
What is unilateral tinnitus?
In plain language, unilateral tinnitus is the perception of soundoften a ringing, buzzing, or hissingthat occurs in only one ear. It differs from the more common bilateral tinnitus, where both ears are affected. This distinction matters because the causes and, consequently, the treatments can be quite different.
Most common cause of unilateral tinnitus
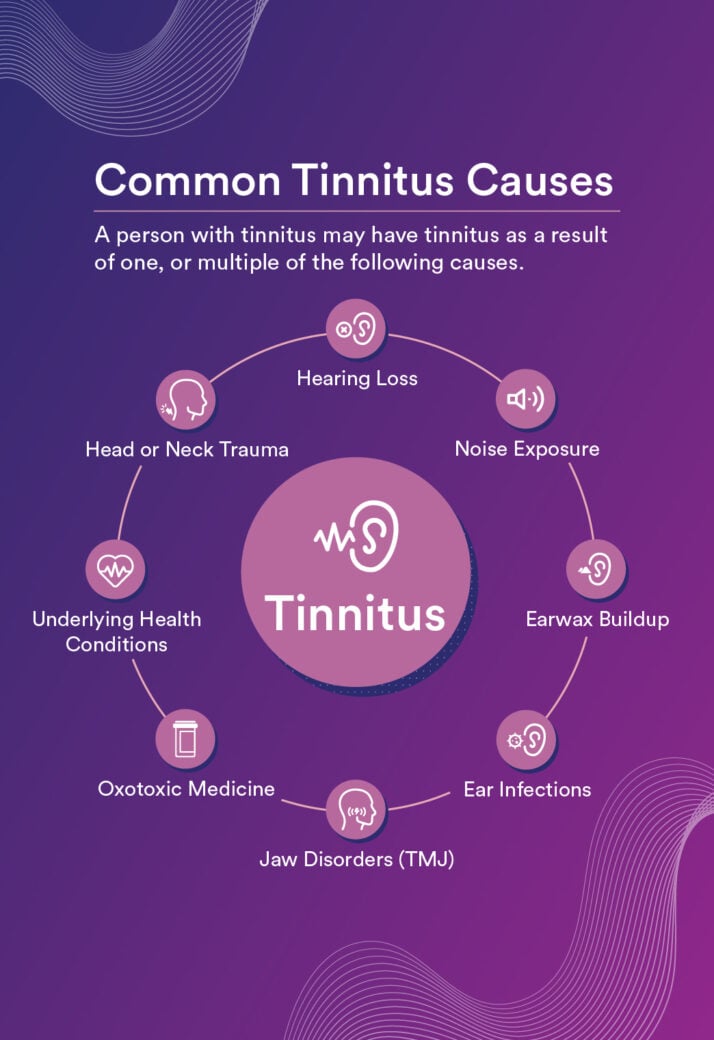
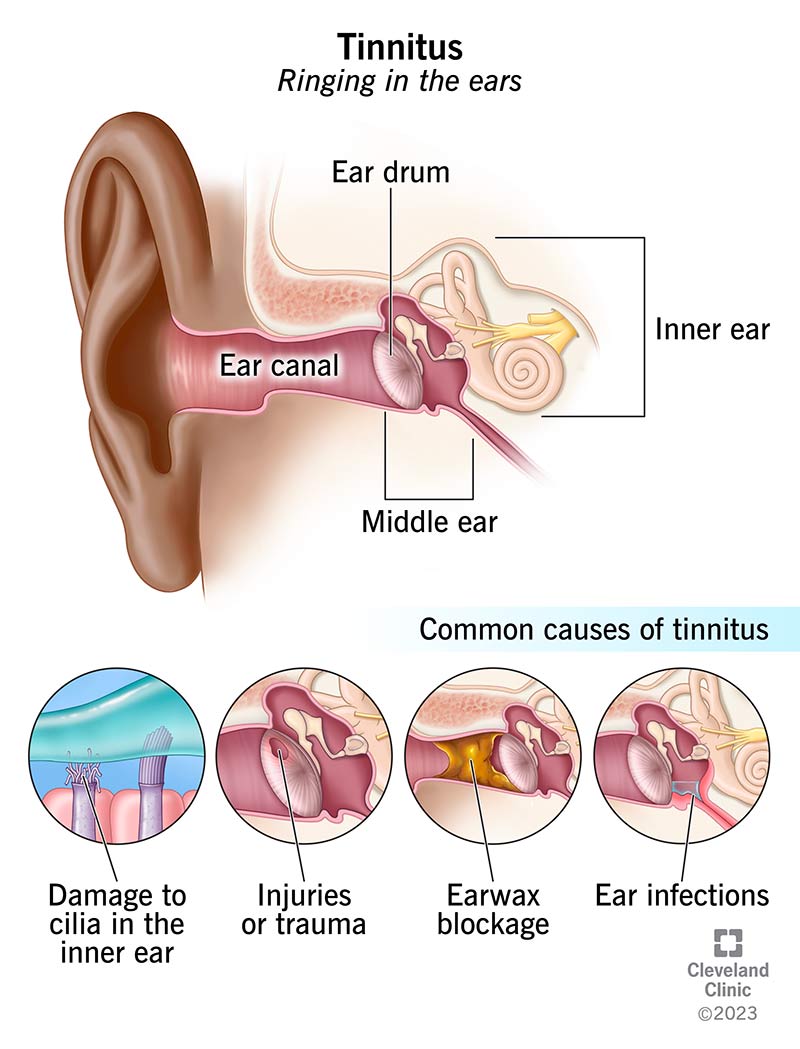
When doctors look at the data, the top culprit is a simple buildup of earwax (cerumen). A blocked ear canal can trap sound and create that irritating ring. Following that, infections of the middle ear (like otitis media) and vascular abnormalities that cause pulsatile sounds rank high. A quick glance at the national data shows these three causes cover roughly 7080% of cases.
Is unilateral tinnitus dangerous?
Most of the time, it's not a life-threatening issue. However, certain red-flag signs do demand prompt medical attention: sudden onset, accompanying hearing loss, dizziness, facial weakness, or a rhythmic whoosh that matches your pulse. Those could point to something more serious, like a vascular malformation or a rapidly progressing infection.
Quick differential diagnosis table
| Symptom | Likely cause | First-line test | Typical treatment |
|---|---|---|---|
| Sudden, high-pitched ring | Sensorineural loss | Audiogram | Corticosteroids, hearing aid |
| Pulsatile whoosh | Vascular anomaly | MRI/MRA | Neurosurgical referral |
| Persistent muffled ring + ear fullness | Cerumen impaction | Otoscopic exam | Manual removal, irrigation |
When to Seek Help
Primary-care vs. ENT vs. Audiologist
First stop? Your family doctor. They can rule out common infections or prescribe simple earwax removal. If the ringing persists, they'll likely send you to an ear, nose, and throat (ENT) specialist, who can conduct a full otoscopic exam, tympanometry, and order imaging if needed. An audiologist steps in when hearing loss is suspectedthey'll run detailed hearing tests and fit hearing aids or sound-masking devices.
Red-flag scenarios that need urgent ENT review
- Sudden unilateral tinnitus + noticeable hearing loss.
- Pulsatile tinnitus that matches your heartbeat.
- Accompanying vertigo, facial numbness, or weakness.
- Recent head trauma or sudden change after a flight.
In any of these cases, call an ENT within 2448 hours. Early intervention can make a huge difference.
What to expect at your first ENT appointment
When you walk into the clinic, the ENT will generally follow this roadmap:
- History check: When did it start? Any recent infections, injuries, or stressful events?
- Physical exam: Otoscopy to view the ear canal, tympanometry to assess middle-ear pressure.
- Hearing tests: Pure-tone audiometry, speech-in-noise tests.
- Imaging (if needed): A CT or MRI to look for tumors, vascular issues, or inner-ear anomalies.
Depending on findings, you might be referred to a neurologist (for neurological causes) or a radiologist for advanced imaging.
Patient-story snippet
Maria, a 42-year-old teacher, noticed a buzzing in her left ear after a cold. She first tried over-the-counter drops, but the sound persisted. A quick visit to her primary-care doctor led to an ENT referral. An otoscopic exam revealed a solid plug of earwax lodged deep in the canal. After gentle microsuction, the ringing faded within a day. "I felt like the world finally turned down the volume," she laughed, grateful for a simple fix.
Treatment Options Overview
Medical-only treatments (including unilateral tinnitus without hearing loss)
If the cause is something like earwax or an infection, the solution can be surprisingly straightforward:
- Earwax removal: Manual extraction with a curette, microsuction, or gentle irrigationall done by a professional.
- Antibiotics or steroids: For bacterial middle-ear infections or eustachian tube dysfunction, a short course can clear inflammation and silence the ringing.
- Systemic meds for Menire-related tinnitus: Diuretics and low-sodium diets have shown modest benefits, according to a review in the Journal of Otology.
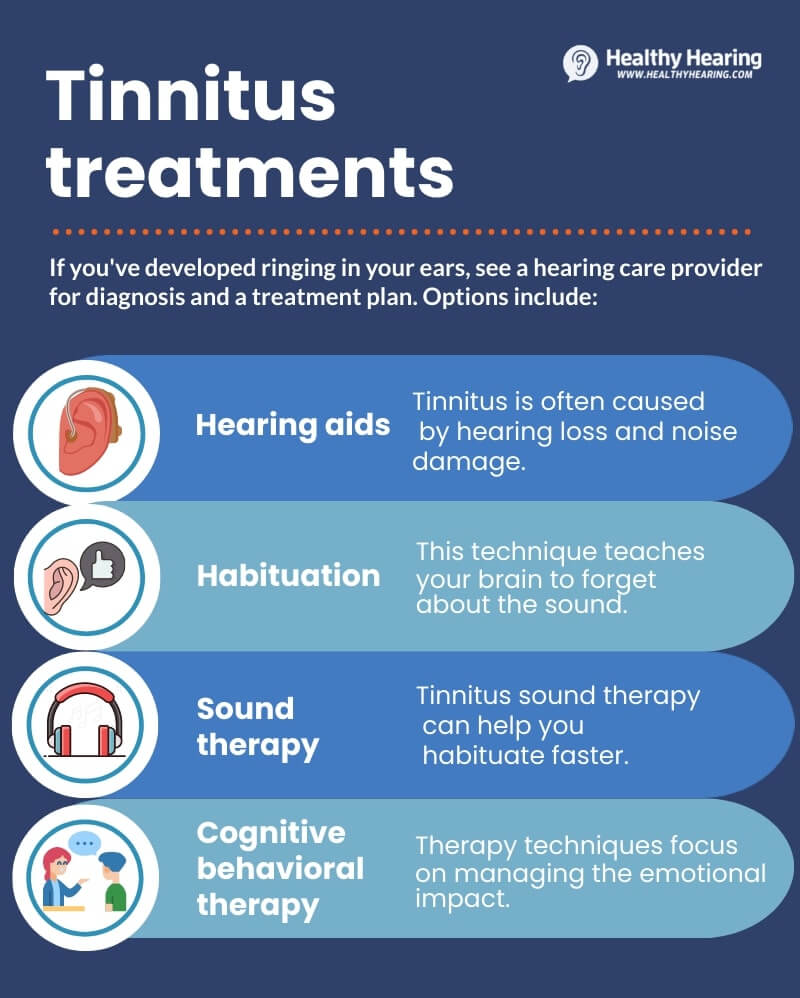
Sound-therapy & hearing aids
When the tinnitus persists despite fixing the underlying cause, maskers come into play. These devices emit low-level white noise that blends with the ringing, making it less noticeable. Modern hearing aids often have built-in sound generators, so you can treat both hearing loss and tinnitus in one package.
Cognitive-Behavioral Therapy (CBT)
CBT doesn't silence the sound, but it reshapes how your brain reacts to it. Studies published by the American Academy of Family Physicians reveal that CBT can reduce tinnitus-related distress by up to 50%. A typical program runs for 612 weekly sessions, focusing on stress-management, relaxation techniques, and thought-reframing.
Surgical interventions
These are reserved for rare, structural causes:
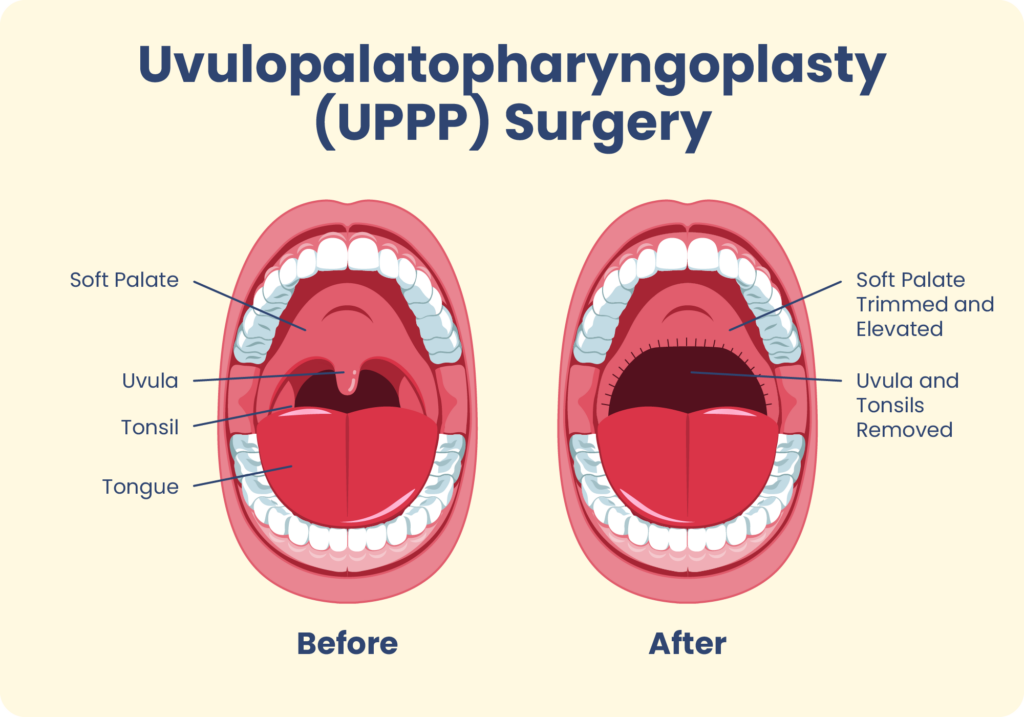
- Cholesteatoma removal: Surgery eliminates the abnormal skin growth that can press on inner-ear structures.
- Vascular lesion repair: For pulsatile tinnitus caused by an arteriovenous malformation, microsurgical correction or endovascular embolization may be required.
- Cochlear implantation: When severe sensorineural loss coexists with tinnitus, a cochlear implant can both restore hearing and suppress the phantom sound.
Lifestyle & home remedies
Sometimes the best aid is a habit change:
- Limit caffeine and alcoholthey can heighten inner-ear activity.
- Practice stress-relief methods like tinnitus meditation, yoga, or deep-breathing exercises.
- Avoid prolonged use of earplugs or headphones at high volume.
Comparison chartWhich treatment fits my situation?
...
Balancing Benefits & Risks
...
Unilateral tinnitus is rarely a mysterious curse; more often it's a signal that something in the earor nearbyneeds care. By pinpointing the root cause, you open the door to targeted treatments ranging from simple earwax removal to advanced surgical repair. Prompt evaluation, especially when red-flag symptoms appear, ensures dangerous conditions are ruled out and the most effective plan is set in motion.
So, if you've been living with that one-ear ring, don't just push it to the background. Book that appointment, keep a short diary, and remember there's a road map to relief. Have you tried any of these steps, or do you have a story you'd like to share? Drop a comment, ask a question, or simply let us know how you're feeling. Your experience could help someone else find the quiet they've been searching for.
FAQs
What is the most common cause of unilateral tinnitus?
Earwax (cerumen) buildup is the leading cause, accounting for the majority of single‑ear ringing cases.
When should I see an ENT specialist for unilateral tinnitus?
If the ringing is sudden, accompanied by hearing loss, dizziness, facial weakness, or a pulsatile “whoosh” sound, seek ENT care within 24‑48 hours.
Can unilateral tinnitus be treated without medication?
Yes. Simple ear‑wax removal, sound‑masking devices, and cognitive‑behavioral therapy can effectively reduce or eliminate the ringing.
Are there surgical options for unilateral tinnitus?
Surgery is reserved for structural causes such as cholesteatoma, vascular malformations, or when a cochlear implant is indicated for severe sensorineural loss.
How does a tinnitus diary help in treatment?
Tracking intensity, triggers, stress levels, and sleep patterns for two weeks helps clinicians identify patterns and tailor the most effective treatment plan.