Most adrenal nodules turn out to be harmless, but because they can sometimes secrete hormones or, in rare cases, be malignant, doctors usually run a few quick tests to be sure. In the next few minutes we'll walk through what the size means, what (if any) symptoms to watch for, and what the typical next-step tests and treatments are so you can feel confident at your next appointment.
Adrenal Nodule Basics
What counts as a nodule?
A nodule is simply a small, roundish spot that shows up on imaging (CT, MRI, or ultrasound). In the adrenal gland it's often called an incidentaloma because it's discovered when doctors are looking for something else. The term tumor can sound scary, but most of these lesions are noncancerous growths called adenomas.
How common are they?
Studies estimate that up to 7% of people over 50 will have an adrenal incidentaloma on a routine scan. Most of those never cause any problems.
Quick Fact Box
| Typical Size | Usual Significance | Typical Management |
|---|---|---|
| 1cm (10mm) | Very small, almost always benign | Followup imaging in 12months |
| 2cm | Benign in >90% of cases | Hormone labs + repeat scan |
| 4cm | Higher risk of malignancy or hormone excess | Consider surgical removal |
Size and Significance
Why does a 1cm nodule feel less scary?
A 1cm (10mm) left adrenal nodule is tinyabout the size of a pea. At that size the chances of it being a cancerous lesion are below 2%. Doctors usually just keep an eye on it with a repeat scan a year later.
What about a 2cm nodule?
A 2cm adrenal nodule is still likely benign, but it nudges the odds up a bit. That's why most endocrinologists order a panel of hormone tests (cortisol, aldosterone, metanephrines) to rule out a functional adenoma that might be secreting excess hormones.
When does size become a red flag?
When a nodule reaches 4cm or larger, the calculus changes. Larger lesions are more likely to be hormonally active or, in a minority of cases, malignant. Your doctor may suggest a more detailed imaging study (like an MRI with fat-suppression) or even a biopsy if the imaging is ambiguous.
Size Comparison Table
| Size | Benign Likelihood | Typical Action |
|---|---|---|
| 1cm (10mm) | 98% | Annual imaging |
| 2cm | 92% | Lab work + followup |
| 3cm | 85% | Closer imaging + labs |
| 4cm | 60% (higher risk) | Consider surgery |
Symptoms to Watch
Most nodules stay silent
In reality, the majority of adrenal nodules never cause any symptoms. That's why they're often called incidentalomasyou discover them while looking for something else, like a kidney stone.
Hormone-related signs
If a nodule is functional, it can overproduce hormones. Here's a quick cheatsheet of what you might feel:
- Cortisol excess - weight gain around the belly, easy bruising, fatigue.
- Aldosterone excess - high blood pressure, frequent thirst, low potassium.
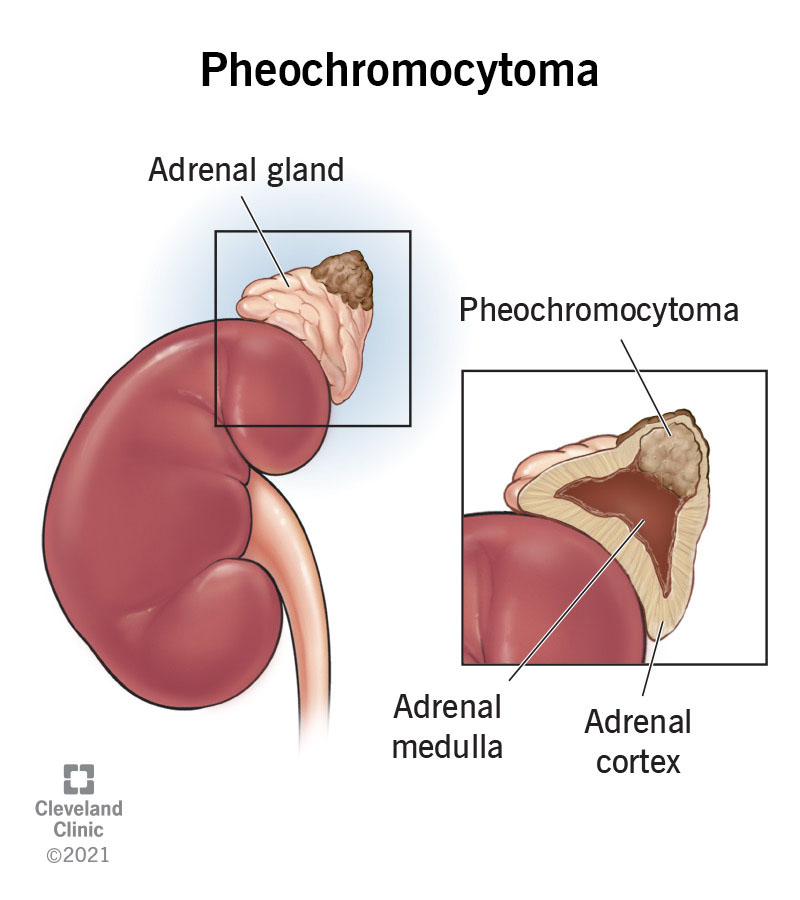
- Catecholamine excess (pheochromocytoma) - rapid heartbeat, sweating, headaches.
Women sometimes notice changes in menstrual cycles, acne, or extra facial hairthese are the adrenal gland tumor symptoms in female that can hint at an androgen-producing adenoma.
Real-world story
Take Jane, a 42-year-old teacher who went in for a routine CT after a minor car accident. The radiologist reported a 2cm nodule on her right adrenal gland. Jane felt perfectly fineuntil a few weeks later she started feeling unusually tired and noticed a new moon face. A simple blood test revealed mildly elevated cortisol, and her physician explained that the nodule was likely secreting excess hormone. A short course of medication helped stabilize her levels, and a followup scan showed the nodule unchanged. Jane's story illustrates how a seemingly silent finding can sometimes whisper its presence.
How Doctors Evaluate
Blood work first
After the imaging shows a nodule, most endocrinologists order a set of hormone panels:
- 24-hour urinary free cortisol or midnight salivary cortisol (to check cortisol excess).
- Plasma aldosterone concentration and renin activity (to assess aldosterone excess).
- Plasma or urinary metanephrines (to rule out pheochromocytoma).
These tests are quick, inexpensive, and give a clear picture of whether the nodule is functional.
Imaging followup
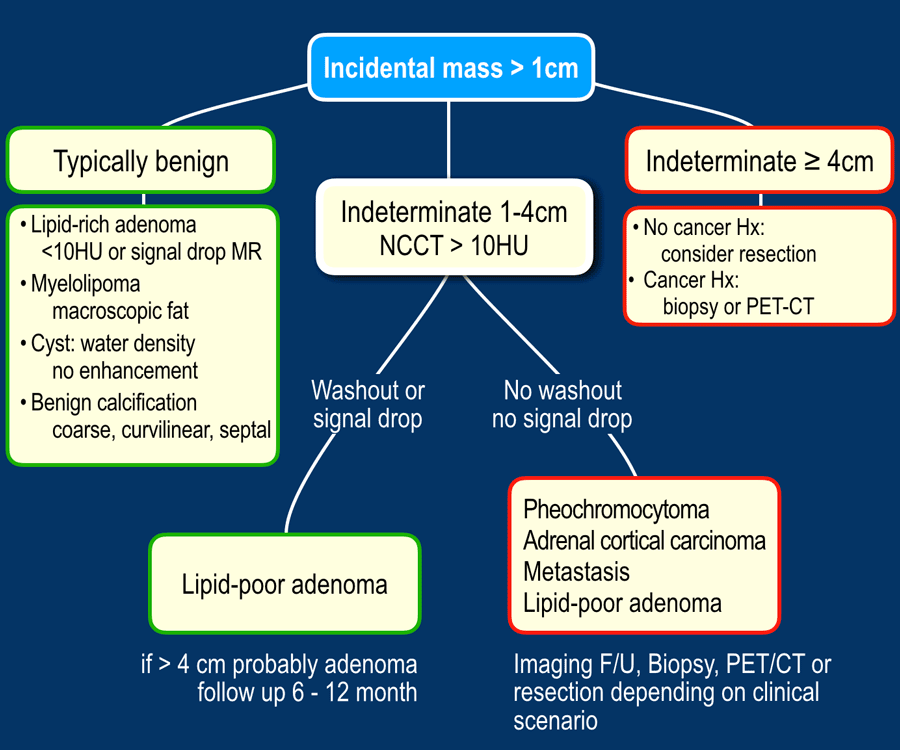
CT attenuation values (measured in Hounsfield units) help differentiate benign adenomas (usually <10HU) from potentially malignant lesions. An MRI with chemical shift can also reveal fatty adenomas, which are almost always benign.
When is a biopsy needed?
Adrenal biopsies are rarely performed because they carry a risk of bleeding and often don't change management. They're usually reserved for cases where imaging and labs are inconclusive, and the lesion is suspected to be metastatic disease from another primary tumor.
Decision-Tree Flowchart (text version)
Imaging Nodule 1cm? - Observe, repeat scan in 12 months.
2cm Nodule <4cm? - Hormone panel. If normal - Repeat imaging in 612 months; if abnormal - Consider surgery or medication.
Nodule 4cm? - Advanced imaging + hormone panel. Discuss surgical removal (laparoscopic adrenalectomy).
Treatment Options Overview
Watchful waiting
If the nodule is small, nonfunctional, and shows no growth, most doctors recommend watchful waiting. That means a repeat CT or MRI in 612 months, plus the occasional hormone check.
Medication for functional nodules
When a nodule secretes excess hormones, medicines can block the hormone's effects. For example, spironolactone can control aldosterone excess, while ketoconazole or metyrapone may dampen cortisol production. These drugs are usually a bridge to surgery, but some patients stay on them indefinitely if surgery isn't an option.
Surgical removal
Adrenal tumor size and growth are key considerations when planning surgery. Laparoscopic adrenalectomy is the gold-standard for nodules that are large (4cm), growing, or hormonally active. Recovery is typically 12 weeks for most daily activities, with fuller recovery over several weeks, and many patients experience immediate symptom relief if the tumor was hormone-producing.
Pros & Cons Table
| Option | Invasiveness | Success Rate | Recovery Time |
|---|---|---|---|
| Watchful Waiting | Noninvasive | Depends on nodule behavior | None |
| Medication | Oral/IV | High for symptom control | Variable (side-effects possible) |
| Surgery | Minimally invasive (laparoscopic) | >95% for benign adenomas | 112 weeks depending on activity |
Practical Visit Checklist
Documents to bring
Before you head to the endocrinology office, gather these items:
- Copy of the latest CT or MRI report (with images if possible).
- List of current medications, including over-the-counter supplements.
- Journal of any symptoms you've noticedeven if they seem unrelated.
Questions to ask your doctor
Don't be shyhere are some conversation starters:
- Do my hormone labs look normal, or should we repeat them?
- What would make you recommend surgery versus observation?
- How often should we repeat imaging, and what changes would prompt a different approach?
- Are there lifestyle adjustments that can help keep my adrenal health stable?
Printable checklist
Think of this as your adrenal nodule cheat sheet. You can copy it onto a sticky note or print it out for your next appointment.
Trusted Resources
Medical sites you can rely on
When you're scrolling through a sea of information, stick to sources that cite peer-reviewed research and professional guidelines.
Support communities
Connecting with others who have walked the same path can be reassuring. Consider joining patient groups and forums focused on adrenal conditions. They're great places to ask practical questions and share experiences.
Spotting misinformation
Be wary of sites that promise quick fixes or claim that every adrenal nodule is a cancer. Reliable articles will reference guidelines from the Endocrine Society or the American Association of Clinical Endocrinology and will be transparent about the limits of current knowledge.
Conclusion
In short, most adrenal noduleswhether they're 1cm, 2cm, or even a bit largerturn out to be harmless. The key is to let your doctor check the hormone picture and keep an eye on the size over time. By staying informed, asking the right questions, and following a clear checklist, you'll turn an unsettling scan result into a manageable part of your health journey. If anything in this guide sparked a question, or if you've already navigated an adrenal nodule and want to share your story, drop a comment below. Your experience could be the reassurance someone else needs.
FAQs
What is an adrenal incidentaloma?
An adrenal incidentaloma is a nodule discovered unintentionally on imaging performed for another reason. Most are benign adenomas.
When does a nodule size become worrisome?
Nodules 4 cm or larger have a higher risk of being malignant or hormonally active, often prompting further imaging or surgery.
What symptoms suggest a hormone‑producing adrenal nodule?
Signs can include unexplained weight gain, high blood pressure, rapid heartbeat, sweating, or changes in menstrual cycles, depending on the hormone involved.
What tests do doctors use to evaluate an adrenal nodule?
Typical work‑up includes blood or urine tests for cortisol, aldosterone, and metanephrines, plus imaging characteristics like Hounsfield units on CT.
Is surgery always required for adrenal nodules?
No. Small, non‑functional nodules are usually observed with periodic scans. Surgery is considered for large, growing, or hormone‑secreting lesions.