Got a sudden hoarse voice, a breathy whisper, or trouble hitting those high notes? You might be dealing with recurrent laryngeal nerve paralysisthe condition that throws your vocal cords out of sync. Below you'll find the straightforward facts about what causes it, how to spot it early, and the best ways to get your voice (and breathing) back on track, all explained in a friendly, no-jargon style.
Understanding the Nerve
What is the recurrent laryngeal nerve?
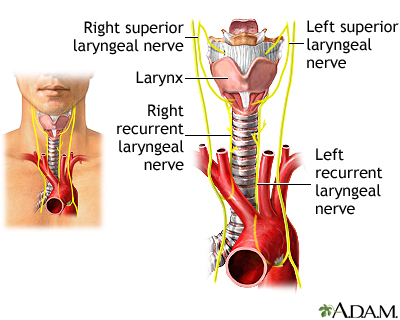
The recurrent laryngeal nerve (RLN) is a tiny, but mighty, branch of the vagus nerve. It loops down around the aorta on the left side and around the subclavian artery on the right before shooting back up to control the muscles that open and close your vocal cords. In plain English, it's the wire that lets you speak, sing, and breathe without straining.
How does paralysis happen?
Paralysis occurs when the RLN is damaged or compressed. The most common culprits are:
- Surgical traumaespecially during thyroidectomy or neck dissection (see Uvula removal for related procedures).
- Tumors or enlarged lymph nodes that press on the nerve.
- Inflammation or infectionrarely, severe thyroiditis or even intubation injuries.
When the damage is only partial, you might notice a slight hoarseness; a complete injury can leave one or both vocal folds frozen in place.
Unilateral vs. bilateral injurywhat's the real difference?
Imagine your vocal cords as a pair of doors. If only one door sticks (unilateral injury), you still get air through the other, but the voice sounds raspy and breathy. If both doors jam (bilateral injury), breathing becomes a struggle and you may even need emergency airway support.
| Feature | Unilateral RLN Injury | Bilateral RLN Injury |
|---|---|---|
| Typical Symptoms | Hoarseness, breathy voice, occasional coughing | Stridor, severe shortness of breath, voice may be barely audible |
| Urgency | Prompt ENT evaluation | Immediate airway assessment; possible tracheostomy |
| Treatment Focus | Voice restoration | Airway protection first, voice later |
Spotting the Signs
What are the hallmark symptoms?
The RLN controls both vocal cord movement and airway protection, so its injury shows up in two main ways:
- Voice changesa new hoarseness, a cobblestone sound, or losing the ability to hit high pitches.
- Breathing & swallowing issuesnoisy breathing (stridor), coughing after meals, or the sensation of food sticking.
If you notice any of these after surgery or a recent illness, it's worth getting evaluated sooner rather than later.
How to differentiate from other voice problems?
While RLN palsy makes the voice sound breathy and low, an injury to the superior laryngeal nerve typically robs you of high notes but leaves the low range relatively intact. Think of it as the difference between a muffled speaker (RLN) and a speaker that can't hit the treble (SLN).
Red flags that need urgent attention
Any sudden, loud wheezing (stridor), rapid shortness of breath, or the feeling that you can't get enough air should be treated as an emergency. Bilateral paralysis can progress quickly, and early airway management can be lifesaving.
Diagnosis Steps
Who should perform the exam?
Only a qualified otolaryngologist (ENT) or an experienced speech-language pathologist should examine the larynx. Their training ensures accurate interpretation of what they see.
What tests confirm RLN paralysis?
The gold standard is a flexible fiberoptic laryngoscopya tiny camera slipped through the nose to visualize the vocal cords in motion. If the cords appear stuck, the diagnosis is clear.
Additional tools include:
- Electromyography (EMG) of the laryngeal muscles to gauge nerve activity.
- Voice acoustic analysis software can quantify hoarseness and pitch range.
- Imaging (CT or MRI) helps locate compressive tumors or structural anomalies.
Partial vs. complete classification
During laryngoscopy, a partial injury shows limited movement (the cord wiggles but doesn't close fully). A complete injury means the cord is immobile. This distinction guides treatment decisions.
Treatment Options
Do I always need surgery?
Nope. Many patients experience gradual recovery over weeks to months, especially after a brief stretch or mild compression. During that window, speech therapy and vocal rest are often enough. Speech-language therapy is particularly beneficial, with exercises designed to improve vocal cord function.
Surgical interventionswhat are they?
If the voice remains impaired after three to six months, or if breathing is compromised, surgeons consider:
- Injection laryngoplastya gel is injected into the paralyzed cord to push it toward the midline, improving closure.
- Type I thyroplasty (medialization)a tiny titanium plate adjusts the position of the cord permanently.
- Reinnervationthe surgeon reconnects the damaged RLN to a nearby healthy nerve, hoping the nerve regrows over time.
Each option has its own risk profile. For example, injections are reversible and low-risk but may need repeat procedures, whereas thyroplasty offers lasting results but requires an operation under general anesthesia.
Unilateral vs. bilateral treatment nuances
When only one side is affected, the goal is voice qualityso medialization or injection works well. With bilateral paralysis, the priority shifts to securing a safe airway; sometimes a temporary tracheostomy is placed before any voice-centric surgery.
Emerging therapies and clinical trials
Researchers are exploring nerve grafts and stem-cell techniques that could one day restore full nerve function. While still experimental, a handful of early-phase trials reported promising results in 20242025, suggesting hope for the future.
Living with RLN
Voice hygiene basics
Think of your voice as a delicate instrument; treat it with care:
- Stay hydratedaim for 8 glasses of water a day.
- Use a humidifier, especially in dry climates.
- Avoid shouting, whispering (which strains the cords), and smoking.
Speech-language therapy exercises
Our fellow speech pathologists often recommend glottic closure drills: gently buzzing a low hum while keeping the throat relaxed, then gradually adding syllables (mamama). Consistency (1015 minutes a day) can improve coordination. For complementary holistic approaches, some patients also find relief with tinnitus meditation, which helps reduce stress-related voice tension.
Managing breathing & sleep
If you have bilateral involvement, sleeping propped up or using a CPAP mask (if recommended by your pulmonologist) can keep the airway open. Simple positional changeslike lying on your sidemight also reduce nighttime stridor.
Patient stories (real-world examples)
Case 1: Sarah, a 42-year-old teacher, noticed a raspy voice after thyroid surgery. After three months of voice therapy, she regained 80% of her range without surgery. Case 2: Mark, a 58-year-old mountaineer, developed bilateral RLN paralysis after a severe chest infection. He required a temporary tracheostomy, but within six months, a medialization procedure restored his breathing and gave his voice a respectable quality.
Both stories highlight that recovery can be a marathon, not a sprint, and that a multidisciplinary team (ENT, SLP, pulmonology) often produces the best outcome.
Resources & References
Clinical guidelines & textbooks
For deeper reading, consider the StatPearls chapter on vocal cord paralysis and the American Academy of OtolaryngologyHead and Neck Surgery guidelines (both highly respected sources).
Support groups & advocacy
Online communities such as the Vocal Cord Paralysis Foundation provide peer support, practical tips, and motivation for patients navigating this journey.
When to contact a specialist
If you experience any new hoarseness lasting more than two weeks, sudden breathing difficulty, or swallowing trouble, schedule an ENT appointment promptly. Early intervention often leads to better voice and airway outcomes.
Remember, you're not alone in this. Understanding what's happening to your nerve, recognizing the signs, and partnering with the right specialists can turn a scary situation into a manageable one. If you have questions, share them in the comments or reach out to a trusted healthcare provideryou deserve clear answers and compassionate care.
What's your experience with voice changes after surgery? Have you tried any of the exercises mentioned? Let's keep the conversation going and help each other find the best path forward.
FAQs
What causes recurrent laryngeal nerve paralysis?
The most common causes are surgical trauma (especially thyroid or neck surgery), tumors or enlarged lymph nodes that compress the nerve, and, less often, inflammation, infection, or intubation injury.
How is RLN paralysis diagnosed?
An ENT specialist performs a flexible fiberoptic laryngoscopy to visualize vocal‑cord movement. Additional tests may include laryngeal EMG, acoustic voice analysis, and imaging (CT/MRI) to locate compressive lesions.
What are the treatment options for unilateral RLN paralysis?
Initial management often involves voice therapy and vocal rest. If voice does not improve after 3–6 months, options include injection laryngoplasty, type I thyroplasty (medialization), or nerve re‑innervation procedures.
When is emergency care needed for bilateral RLN paralysis?
Bilateral paralysis can cause airway obstruction. Sudden stridor, severe shortness of breath, or inability to speak clearly are red‑flag signs that require immediate airway assessment, possibly a tracheostomy, before any voice‑focused treatment.
Can the voice improve after RLN paralysis without surgery?
Yes, many patients experience partial or full recovery within weeks to months, especially if the injury is due to stretch or temporary compression. Consistent speech‑language therapy and proper voice hygiene greatly enhance recovery chances.