If youve just learned that your thyroid isnt doing its job, the first thing you probably want to know is: how will I be treated? The short answer is that the treatment depends on where the problem starts the thyroid itself (primary) or the brains pituitaryhypothalamic axis (secondary). Both require hormone replacement, but the dosing, lab targets, and followup differ enough that a onesizefitsall approach can miss the mark.
Below well walk through the two types of hypothyroidism, the labs that tell them apart, the exact steps doctors take to get you feeling better, and some realworld stories that show why the details matter. By the end youll have a clear picture of what to expect, what questions to ask, and how to stay in control of your health.
Understanding the Types
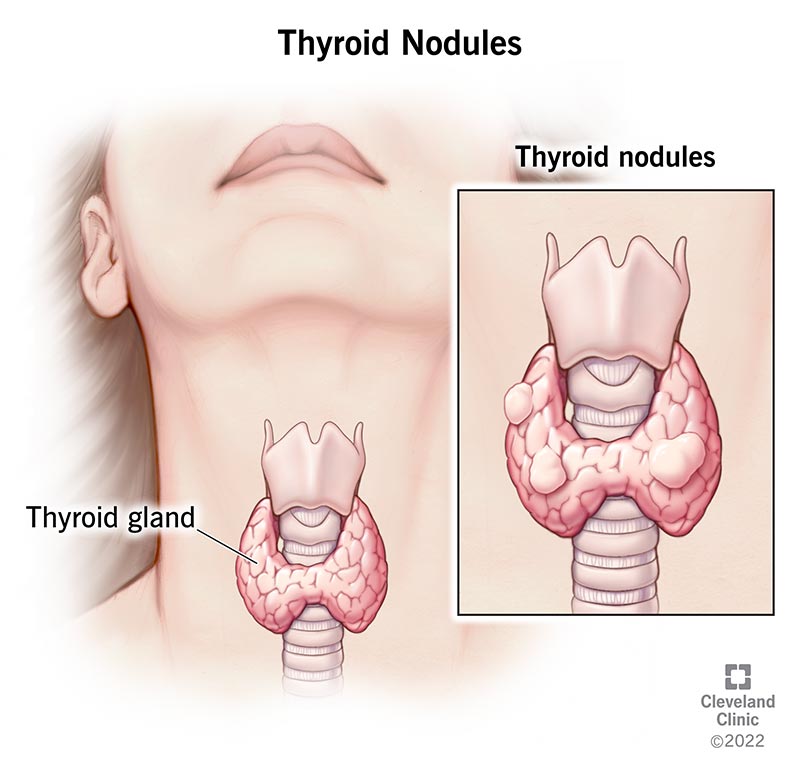
What Is Primary Hypothyroidism?
Primary hypothyroidism means the thyroid gland itself cant produce enough thyroid hormone. Its the most common form and is often called underactive thyroid. Typical data list the leading causes as:
- Autoimmune attack (Hashimotos thyroiditis)
- Iodine deficiency (rare in the U.S.)
- Thyroidectomy or radiation treatment for cancer
- Rare genetic defects
What Is Secondary (Central) Hypothyroidism?
Secondary hypothyroidism isnt a problem with the thyroid itself; its a signaling issue. The pituitary gland or hypothalamus fails to send enough thyroidstimulating hormone (TSH) to the thyroid, so the gland stays quiet. Common triggers include:
- Pituitary tumors or surgery
- Radiation to the brain
- Sheehans syndrome (postpartum pituitary infarction)
- Rare infiltrative diseases
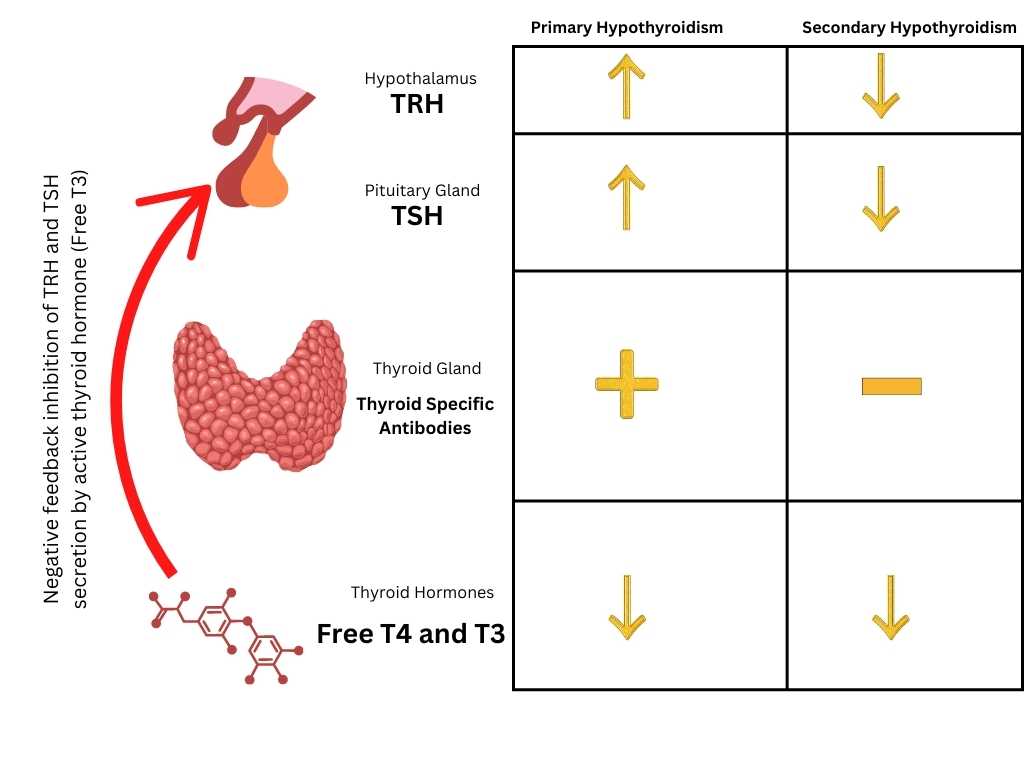
Quick Lab Snapshot
| Lab Test | Primary | Secondary | Typical Range | Interpretation |
|---|---|---|---|---|
| TSH | High | Low or normallow | 0.44.0mIU/L | Controls thyroid hormone production |
| FreeT4 | Low | Low | 0.81.8ng/dL | Active thyroid hormone |
| Cortisol/ACTH | Usually normal | May be low if other pituitary axes involved | Varies | Screen for panhypopituitarism |
Treatment Goals Overview
What Both Types Want to Achieve
Regardless of cause, the goals are the same:
- Relieve symptoms (fatigue, cold intolerance, weight changes)
- Normalize thyroidhormone levels in the bloodstream
- Prevent longterm complications like heart problems, high cholesterol, or myxedema
Why One Size Doesnt Fit All
In primary hypothyroidism the bodys natural feedback loop (high TSH tells the doctor youre still low) works well, so doctors can finetune levothyroxine based on TSH. In secondary cases, TSH is unreliable; the pituitary isnt shouting the right numbers, so clinicians rely on FreeT4 and the patients clinical picture. This difference means the dosing, monitoring frequency, and even the risk profile can diverge dramatically.
Primary Hypothyroidism Care
FirstLine: Levothyroxine
Levothyroxine (brand names Synthroid, Levoxyl, etc.) is the gold standard. A typical starting dose is about 1.6g per kilogram of body weight per day, but doctors will lower it for older adults, people with heart disease, or those who are pregnant.
How To Titrate
After the first prescription, youll usually get a followup TSH test in 68weeks. If your TSH is still high, the dose goes up a bit; if its low, the dose comes down. Once you land in the target range (roughly 0.52.0mIU/L), most clinicians space out testing to every six months.
Alternatives & Adjuncts
- Liothyronine (T3) sometimes added for patients who feel sluggish despite a normal TSH.
- Combination therapy (T4+T3) still debated; a review notes it may help a minority of patients but isnt firstline.
Lifestyle Support (Hypothyroidism Diet)
While medication does the heavy lifting, certain foods can support thyroid health:
- Iodinerich foods (seaweed, dairy, eggs) but avoid megadoses unless prescribed.
- Seleniumrich foods (Brazil nuts, sunflower seeds) aid hormone conversion.
- Limit soy and cruciferous veggies if you eat them raw in massive amounts; cooking reduces goitrogenic effects.
Remember, a hypothyroidism diet alone wont replace hormone therapy, but it can smooth the journey.
Practical Checklist for Primary Patients
- Take levothyroxine on an empty stomach, same time each day.
- Avoid calcium or iron supplements within four hours of the dose.
- Keep a simple symptom diary note energy, mood, weight, and any new aches.
Secondary Hypothyroidism Care
Levothyroxine Still Leads, But Dosing Shifts
Because TSH can be misleading, doctors target a FreeT4 level of about 0.91.4ng/dL. The usual starting dose is lower roughly 1.0g/kg/day and its adjusted based on FreeT4 rather than TSH.
Monitoring Frequency
In the first few months, FreeT4 is checked every 46weeks until it steadies. Once stable, labs can be spaced out to every 612months. Some endocrinologists still look at TSH for a rough guide, but they emphasize that a low TSH doesnt mean youre overtreated.
Dont Forget the Rest of the Pituitary
If your pituitary is offbalance, you might also have low cortisol, growth hormone, or sex hormones. Before starting levothyroxine, clinicians often screen cortisol and ACTH to avoid triggering an adrenal crisis. Treating the underlying pituitary issue (surgery, radiation, or hormone replacement) is a parallel priority.
Common Pitfalls & Fixes
| Pitfall | Why It Happens | How to Fix It |
|---|---|---|
| Relying on TSH alone | TSH is low/normal in secondary disease | Base dose changes on FreeT4 and symptoms |
| Missing adrenal insufficiency | Pituitary disorders often affect cortisol | Check cortisol before levothyroxine; replace if needed |
| Inconsistent dosing time | Absorption varies with food and other meds | Take pill with water, same hour daily, avoid calcium/iron |
When Might You Need T3?
Some secondary patients report lingering fatigue even when FreeT4 looks good. A lowdose T3 addition can be considered, but only under close endocrinology supervision because T3 has a shorter halflife and can cause spikes.
SidebySide Comparison
Dosing & Titration
- Primary: TSHguided; starting dose 1.6g/kg; adjustments every 68weeks.
- Secondary: FreeT4guided; starting dose 1.0g/kg; adjustments every 46weeks.
Lab Monitoring
- Primary TSH primary marker, free T4 secondary; annual labs after stable.
- Secondary FreeT4 primary; TSH low/normal, used only for reference.
Risk Profile
| Risk | Primary | Secondary |
|---|---|---|
| Overtreatment (Afib, osteoporosis) | Higher if TSH overshoots | Lower if FreeT4 kept in range |
| Undertreatment (cognitive slowdown) | Possible if dose too low | Possible if pituitary issue ignored |
| Hidden adrenal insufficiency | Rare | More common screen early |
Downloadable Cheat Sheet
For quick reference, you can copy this table into a note on your phone. Its a handy reminder before every doctors visit.
RealWorld Stories
Jennys Journey Primary
Jenny, a 34yearold teacher, noticed persistent fatigue, hair loss, and a cold feeling even in summer. Her doctor ordered a TSH of 12mIU/L and a FreeT4 of 0.6ng/dL classic primary hypothyroidism. She started on 100g levothyroxine, took it each morning with water, and avoided her calcium supplement for four hours. After six weeks her TSH dropped to 3.2, and her energy bounced back. She now checks her labs yearly and keeps a simple diary that notes any brain fog.
Marks Puzzle Secondary
Mark, 48, underwent surgery for a pituitary macroadenoma two years ago. Postop labs showed a low TSH (0.2) and low FreeT4 (0.9). He was diagnosed with secondary hypothyroidism. His endocrinologist started him on 75g levothyroxine, targeting a FreeT4 of 1.1. At the same time, Marks cortisol was borderline, so he received a lowdose hydrocortisone. Six weeks later his FreeT4 was perfect, but he still felt sluggish. After a careful discussion, a tiny 5g T3 dose was added, smoothing out the energy dip. Mark now has a schedule: levothyroxine each morning, T3 at lunch, and cortisol with breakfast if his stress level spikes.
Quick Answers (FeaturedSnippet Style)
Can both types be treated with the same medication?
Yes. Levothyroxine is the firstline therapy for both primary and secondary hypothyroidism, but the dose, lab target, and monitoring frequency differ.
What lab values indicate secondary hypothyroidism?
Low or inappropriately normal TSH combined with a low FreeT4, often accompanied by abnormal ACTH or cortisol if other pituitary hormones are affected.
Is a hypothyroidism diet enough to replace medication?
No. Diet can support thyroid health, but it cannot generate the hormones your body needs. Medication remains essential for symptom control and longterm safety.
How long will I need medication?
Primary hypothyroidism is typically lifelong. Secondary hypothyroidism may also be lifelong, unless the underlying pituitary problem resolves completely, which is uncommon.
Action Steps & Resources
Checklist Before Your Next Appointment
- Bring the most recent TSH, FreeT4, and, if secondary, cortisol results.
- Write down every medication, supplement, and overthecounter product.
- Note any new symptoms weight change, mood swings, heart palpitations.
- Prepare questions: Should we adjust my dose based on FreeT4? Do I need an adrenal test?
Trusted Sources for Further Reading
When to Call the Doctor Immediately
If you notice rapid weight gain, facial swelling, severe fatigue, shortness of breath, or a racing heartbeat, seek medical attention right away. These could be signs of overtreatment or worsening hypothyroidism.
Understanding the nuances between primary and secondary hypothyroidism treatment can feel like decoding a secret code, but you dont have to do it alone. Keep these tables, checklists, and stories handy, ask the right questions, and stay proactive about your labs. Your thyroid may be undertalking, but with the right plan you can turn the conversation back up to a comfortable volume.
Got a question about your own lab results or how to fit medication into a busy day? Im here to helpjust reach out to your healthcare provider and bring this guide along for reference. You deserve clear answers, steady energy, and peace of mind.
FAQs
What is the main difference in treatment between primary and secondary hypothyroidism?
Both types are treated with levothyroxine hormone replacement, but primary hypothyroidism dosing and monitoring are guided mainly by TSH levels, while secondary hypothyroidism relies on FreeT4 levels and clinical symptoms due to unreliable TSH.
How are levothyroxine doses adjusted in primary vs secondary hypothyroidism?
In primary hypothyroidism, doses start around 1.6 μg/kg/day and are adjusted based on TSH every 6–8 weeks. In secondary hypothyroidism, doses start lower at about 1.0 μg/kg/day and are adjusted every 4–6 weeks based on FreeT4 levels.
Why is TSH an unreliable marker in secondary hypothyroidism?
Secondary hypothyroidism is caused by pituitary or hypothalamic dysfunction, which impairs TSH secretion, causing low or inappropriately normal TSH despite low thyroid hormone levels, so FreeT4 and symptoms are primary monitoring tools.
Can diet alone treat hypothyroidism?
No, diet can support thyroid health but cannot replace hormone replacement therapy, which is essential in both primary and secondary hypothyroidism for symptom control and preventing complications.
Do patients with secondary hypothyroidism need additional hormone tests?
Yes, because pituitary dysfunction may cause deficiencies in other hormones like cortisol, it is important to test adrenal function (cortisol/ACTH) before starting levothyroxine to avoid adrenal crisis.