Feeling constantly cold, gaining weight for no reason, or just being exhausted all the time? Those signs can mean your thyroid isnt doing its job right. The quickest way to figure out whats going on is to know where the problem starts inside the thyroid itself (primary) or higher up in the brains pituitary/hypothalamus (secondary). Below we break down the causes, symptoms, lab clues, and treatments so you can tell the two apart without having to sift through endless medical jargon.
What Is Hypothyroidism?
Hypothyroidism simply means low thyroid hormone. Your thyroid gland, a butterflyshaped organ in the front of your neck, makes two hormones T4 (thyroxine) and T3 (triiodothyronine) that keep your metabolism humming. When those hormones dip, everyday processes slow down, leaving you feeling sluggish, chilly, and sometimes a bit foggy.
Why does the type matter? Because the source of the shortage determines which lab values will be abnormal, which other hormones might be involved, and ultimately how doctors treat you. Knowing the difference empowers you to ask the right questions at the doctors office.
Primary vs Secondary
| Aspect | Primary Hypothyroidism | Secondary (Central) Hypothyroidism |
|---|---|---|
| Origin | Thyroid gland itself | Pituitary or hypothalamus |
| Typical TSH | High (elevated) | Low or inappropriately normal |
| Typical Free T4 | Low | Low |
| Common Causes | Autoimmune (Hashimoto), iodine deficiency, surgery | Pituitary tumors, radiation, Sheehans syndrome, hypothalamic disease |
Think of primary hypothyroidism as a factory malfunction: the thyroid (the factory) cant produce enough product, so the manager (TSH) cranks up its signal trying to compensate. In secondary hypothyroidism the manager itself is broken, so even if the factory is perfectly fine, it never gets the produce more order.
How Do Labs Tell the Story?
The threeletter hormone trioTSH, free T4, and free T3acts like a traffic light. In primary disease, TSH lights up bright red (high) while T4 stays dim (low). In secondary disease, the TSH lamp stays off or flickers weakly, but T4 is still low. , a lowornormal TSH with low free T4 is the hallmark of central (secondary) hypothyroidism.
What About Tertiary Hypothyroidism?
Tertiary hypothyroidism is the rarest siblingit originates in the hypothalamus, the part of the brain that tells the pituitary what to do. Because its so uncommon, most clinicians lump it under secondary for practical purposes, but its worth knowing the term when you see it on a lab report.
Causes & Risks
Primary Hypothyroidism Causes
- Autoimmune Hashimotos thyroiditis the most frequent cause in the U.S.
- Iodine deficiency still a problem in some lowiodine regions.
- Postsurgical or radioactive iodine treatment for hyperthyroidism.
- Medications such as lithium or amiodarone.
Secondary Hypothyroidism Causes
- Pituitary adenoma or craniopharyngioma a benign tumor pressing on hormoneproducing cells.
- Radiation therapy to the head/neck.
- Sheehans syndrome postpartum pituitary infarction after severe bleeding.
- Infiltrative diseases (e.g., sarcoidosis, Langerhans cell histiocytosis).
RealWorld Example
Sarah, a 42yearold mother, lost a lot of blood during a complicated delivery. Months later she felt unusually tired, her milk supply dropped, and routine labs showed low TSH with low T4. The diagnosis? Secondary hypothyroidism from Sheehans syndrome. Her story illustrates why a low TSH isnt always good it can be a warning flag that the pituitary isnt doing its job.
Symptoms Overview
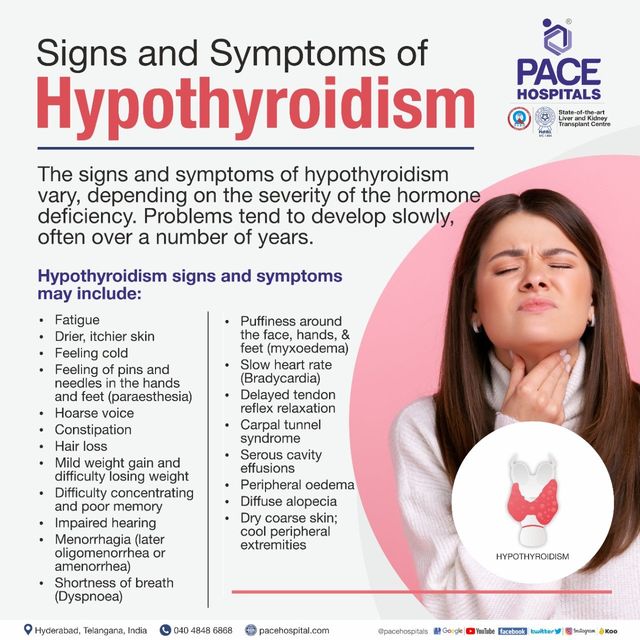
Shared Symptoms (Both Types)
Fatigue, weight gain, dry skin, hair loss, constipation, and a general feeling of being in slow motion. The overlap is why you need lab clues to separate them.
Clues Pointing to Primary
- Visible goiter (enlarged thyroid)
- High cholesterol or LDL levels
- Cold intolerance that worsens in winter
- Elevated TSH on routine screening
Clues Pointing to Secondary
- Other pituitary hormone deficiencies (low cortisol, low sex hormones)
- Symptoms of adrenal insufficiency (dizziness, low blood pressure)
- Normal or low TSH despite clear hypothyroid signs
- History of brain surgery, radiation, or severe postpartum hemorrhage
| Feature | Primary | Secondary |
|---|---|---|
| TSH | High | Low/Normal |
| Free T4 | Low | Low |
| Goiter | Often present | Rare |
| Other hormone issues | Uncommon | Frequent |
Diagnosis Steps
Standard Thyroid Panel
Firstline testing includes TSH, free T4, and sometimes free T3. If TSH is high and free T4 is low, primary hypothyroidism is likely. If TSH is low/normal with low free T4, youre looking at secondary (or tertiary) disease.
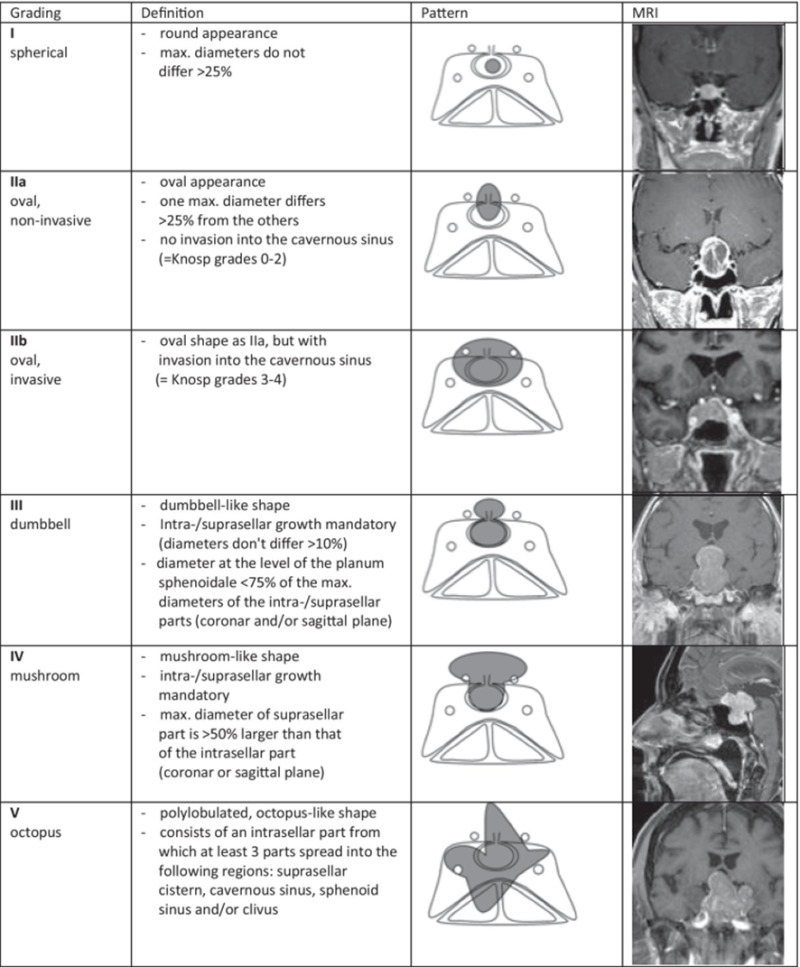
When to Order Pituitary Imaging
Any patient with a low or inappropriately normal TSH plus clinically significant hypothyroid symptoms should get a pituitary MRI. Red flags include visual field changes, headaches, or known pituitary lesions. recommends imaging as soon as central hypothyroidism is suspected.
Subclinical Hypothyroidism
When TSH is mildly elevated (usually 4.510mIU/L) but free T4 stays normal, we call it subclinical hypothyroidism. Its almost always a primary issue and often monitored rather than treated right away, unless the patient has symptoms, is pregnant, or has cardiovascular risk factors.
Treatment Options
Primary Hypothyroidism Treatment
Levothyroxinesynthetic T4is the gold standard. Doses start around 1.6g/kg daily for otherwise healthy adults, then titrated to keep TSH within the normal range. Regular blood tests every 68 weeks after dose changes help finetune the amount.
Secondary Hypothyroidism Treatment
Levothyroxine is still used, but the target shifts. Because TSH cant be trusted as a marker, doctors aim for a normal free T4 (often 1.01.8ng/dL). In addition, any underlying pituitary problem must be addressedsurgery for a tumor, hormone replacement for adrenal insufficiency, or careful monitoring after radiation.
When considering thyroid replacement options, some patients ask about different formulations and brand choices. For those comparing natural desiccated thyroid vs synthetic options, reading patient experiences can help; for example, see a discussion of Armour thyroid reviews to learn how others describe symptom changes and dosing challenges when switching therapies.
Special Situations
- Pregnancy: Both primary and secondary hypothyroid women need slightly higher levothyroxine doses to protect the babys brain development.
- Elderly: Start low and go slow to avoid overreplacement, which can cause atrial fibrillation.
- Adrenal Insufficiency: Always treat adrenal deficiency first; giving thyroid hormone alone can trigger a crisis.
Quick Dosage Reference
| Age/Condition | Starting Levothyroxine Dose |
|---|---|
| Adult, primary, no heart disease | 1.6g/kgdaily |
| Adult, secondary, pituitary disease | Based on free T4 goal, usually 2550gdaily |
| Older adults (>65y) | Start 2550gdaily |
Hyperthyroidism Contrast
While were focusing on low thyroid function, its useful to glance at the opposite endhyperthyroidism. Primary hyperthyroidism (e.g., Graves disease) originates in the thyroid and shows a low TSH with high T4/T3. Secondary hyperthyroidism, often due to a TSHsecreting pituitary adenoma, presents with high TSH. The primary vs secondary pattern works the same way at both ends of the thyroid spectrum, reinforcing why the source matters.
Takeaway Summary
- Primary hypothyroidism starts in the thyroid high TSH, low T4.
- Secondary hypothyroidism starts in the pituitary/hypothalamus low/normal TSH, low T4.
- Lab patterns are the fastest way to differentiate; imaging is needed when central disease is suspected.
- Treatment overlaps (levothyroxine) but secondary cases require attention to other pituitary hormones and often a different dosing goal.
- Never ignore other symptomsfatigue, low blood pressure, or reproductive changes may hint at a broader hormonal puzzle.
Understanding where the problem begins empowers you to ask the right questions, get the right tests, and receive the most appropriate therapy. If anything in this guide sparked a question or reminded you of a personal experience, feel free to share it in the comments. Were all in this together, and your story could help someone else spot the difference sooner.
Conclusion
So, whether your thyroid issue starts in the gland itself or higher up in the brains control center makes a big difference for diagnosis, treatment, and overall health. By looking at that simple lab trioTSH, free T4, and sometimes free T3you can tell primary from secondary in a heartbeat. If you suspect anything unusual, dont wait: ask your doctor about a pituitary evaluation and make sure all relevant hormones are checked. You deserve clear answers and the right care. Got more questions? Drop a comment below or reach out to your healthcare provideryou deserve to feel your best.
FAQs
What is the main laboratory difference between primary and secondary hypothyroidism?
Primary hypothyroidism shows a high TSH with low free T4, while secondary (central) hypothyroidism presents with low or inappropriately normal TSH and low free T4.
Can secondary hypothyroidism cause a goiter?
Goiter is uncommon in secondary hypothyroidism because the thyroid itself is usually normal; enlargement is more typical of primary disease.
When should a pituitary MRI be ordered for hypothyroidism?
If labs reveal low/normal TSH with low free T4, especially with other pituitary hormone deficiencies or symptoms like headaches, an MRI is recommended to evaluate the pituitary.
How is levothyroxine dosing adjusted for secondary hypothyroidism?
Because TSH is unreliable, dosing aims for a normal free T4 level (usually 1.0‑1.8 ng/dL) rather than targeting TSH normalization.
Is subclinical hypothyroidism usually primary or secondary?
Subclinical hypothyroidism—mildly elevated TSH with normal free T4—is almost always a primary condition and is typically monitored rather than immediately treated.