Ever felt inexplicably tired, chilly, and just off? If your doctor says its hypothyroidism, but the usual blood test isnt the whole story, you might be dealing with pituitary hypothyroidism. In a nutshell, this happens when the pituitary gland cant pump enough thyroidstimulating hormone (TSH), leaving your thyroid sluggish. Below youll find the why, the how, and what you can actually do about itall written like a chat over coffee.
Understanding the Condition
Lets start with the basics. The thyroid and pituitary gland have a classic partnership: the pituitary sits like a tiny maestro in your brain, sending out TSH beats that tell the thyroid to release the hormones T4 and T3. When that maestro gets a cold frontsay, from a tumor or injurythe thyroid never gets its cue, and you end up with secondary or pituitary hypothyroidism. Its different from primary hypothyroidism where the thyroid itself is the problem.
Why does this matter? Because the treatment path and the lab results look distinct. In primary hypothyroidism, TSH soars high trying to shout at a lazy thyroid. In pituitary hypothyroidism, both TSH and free T4 are low, which can throw off a physician whos expecting the classic highTSH picture.
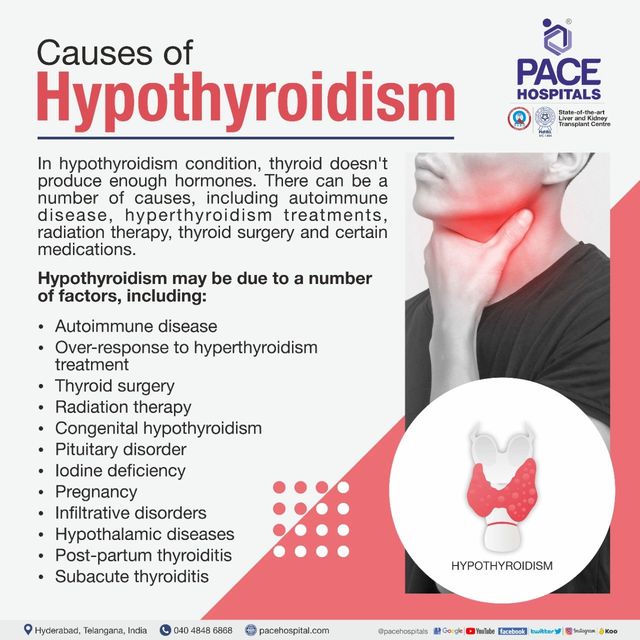
Main Causes
Okay, lets dive into the culprits. Below are the most common pituitary hypothyroidism causes, paired with a quick anecdote so they feel less like textbook bullet points.
Pituitary Tumors (Adenomas)
Picture a small, noncancerous growth perched in the sella turcicathe little bony pocket that houses the pituitary. These adenomas are the #1 cause of secondary hypothyroidism. They can physically compress the gland or secrete other hormones that suppress TSH production.
Imagine Sarah, a 42yearold graphic designer. She started noticing a nagging headache and growing fatigue. Blood work showed low TSH and low free T4. An MRI later revealed a 6mm nonfunctioning adenoma. After a minimally invasive transsphenoidal surgery, her hormone levels normalized, and she got her spark back.
Surgery or Radiation Therapy
Anyone whos had pituitary surgery knows the recovery can be a roller coaster. Even when the surgeons aim is to remove a tumor, the surrounding healthy tissue can be unintentionally affected, impairing TSH output. Radiation (especially fractionated stereotactic radiotherapy) can also gradually damage pituitary cells.
Traumatic Brain Injury (TBI) & Hemorrhage
Blows to the head can bruise the pituitary stalk or its blood supply. A sudden drop in blood flow, known as pituitary apoplexy, can leave the gland underfunctioning. Survivors often report an early fogdifficulty concentrating, feeling coldeven before any hormonal test is done.
Infiltrative Diseases
Conditions like sarcoidosis, hemochromatosis, and Langerhans cell histiocytosis can infiltrate the pituitary, destroying the cells that produce TSH. These diseases are rare, but when they show up, the endocrine system often sends distress signals.
Congenital & Pediatric Causes
Some kiddos are born with a pituitary stalk interruption syndrome or genetic mutations that affect TSH synthesis. In these cases, symptoms may appear earlypoor growth, prolonged jaundice, or persistent low energy.
According to a , around 1520% of secondary hypothyroidism cases are linked to these congenital anomalies.
Recognizing Symptoms
If youre wondering, What does pituitary hypothyroidism feel like? think of a blend between classic hypothy
Understanding the Condition
Lets start with the basics. The thyroid and pituitary gland have a classic partnership: the pituitary sits like a tiny maestro in your brain, sending out TSH beats that tell the thyroid to release the hormones T4 and T3. When that maestro gets a cold frontsay, from a tumor or injurythe thyroid never gets its cue, and you end up with secondary or pituitary hypothyroidism. Its different from primary hypothyroidism where the thyroid itself is the problem.
Why does this matter? Because the treatment path and the lab results look distinct. In primary hypothyroidism, TSH soars high trying to shout at a lazy thyroid. In pituitary hypothyroidism, both TSH and free T4 are low, which can throw off a physician whos expecting the classic highTSH picture.
Main Causes
Okay, lets dive into the culprits. Below are the most common pituitary hypothyroidism causes, paired with a quick anecdote so they feel less like textbook bullet points.
Pituitary Tumors (Adenomas)
Picture a small, noncancerous growth perched in the sella turcicathe little bony pocket that houses the pituitary. These adenomas are the #1 cause of secondary hypothyroidism. They can physically compress the gland or secrete other hormones that suppress TSH production.
Imagine Sarah, a 42yearold graphic designer. She started noticing a nagging headache and growing fatigue. Blood work showed low TSH and low free T4. An MRI later revealed a 6mm nonfunctioning adenoma. After a minimally invasive transsphenoidal surgery, her hormone levels normalized, and she got her spark back.
Surgery or Radiation Therapy
Anyone whos had pituitary surgery knows the recovery can be a roller coaster. Even when the surgeons aim is to remove a tumor, the surrounding healthy tissue can be unintentionally affected, impairing TSH output. Radiation (especially fractionated stereotactic radiotherapy) can also gradually damage pituitary cells.
Traumatic Brain Injury (TBI) & Hemorrhage
Blows to the head can bruise the pituitary stalk or its blood supply. A sudden drop in blood flow, known as pituitary apoplexy, can leave the gland underfunctioning. Survivors often report an early fogdifficulty concentrating, feeling coldeven before any hormonal test is done.
Infiltrative Diseases
Conditions like sarcoidosis, hemochromatosis, and Langerhans cell histiocytosis can infiltrate the pituitary, destroying the cells that produce TSH. These diseases are rare, but when they show up, the endocrine system often sends distress signals.
Congenital & Pediatric Causes
Some kiddos are born with a pituitary stalk interruption syndrome or genetic mutations that affect TSH synthesis. In these cases, symptoms may appear earlypoor growth, prolonged jaundice, or persistent low energy.
According to a , around 1520% of secondary hypothyroidism cases are linked to these congenital anomalies.
Recognizing Symptoms
If youre wondering, What does pituitary hypothyroidism feel like? think of a blend between classic hypothyroid signs and a few extra clues from the pituitary family.
- Fatigue & low energy the classic I could nap forever feeling.
- Cold intolerance even a light sweater feels insufficient.
- Weight gain despite unchanged diet or activity levels.
- Hair loss & dry skin your skin starts craving extra moisturizers.
- Menstrual irregularities or reduced libido because the pituitary also controls sex hormones.
- Adrenal insufficiency symptoms like dizziness upon standing (if other pituitary hormones are low).
When these signs appear together, especially in someone whos already dealing with a pituitary tumor or recent head injury, the suspicion should shift toward secondary hypothyroidism.
Diagnosis Labs
Lab work is the compass that points us in the right direction. Heres the typical pattern youll see for pituitary hypothyroidism:
| Test | Typical Result | Interpretation |
|---|---|---|
| TSH | Low or inappropriately normal | Pituitary not producing enough stimulus. |
| Free T4 | Low | Thyroid not receiving the signal. |
| Free T3 | Low to normal | Depends on peripheral conversion. |
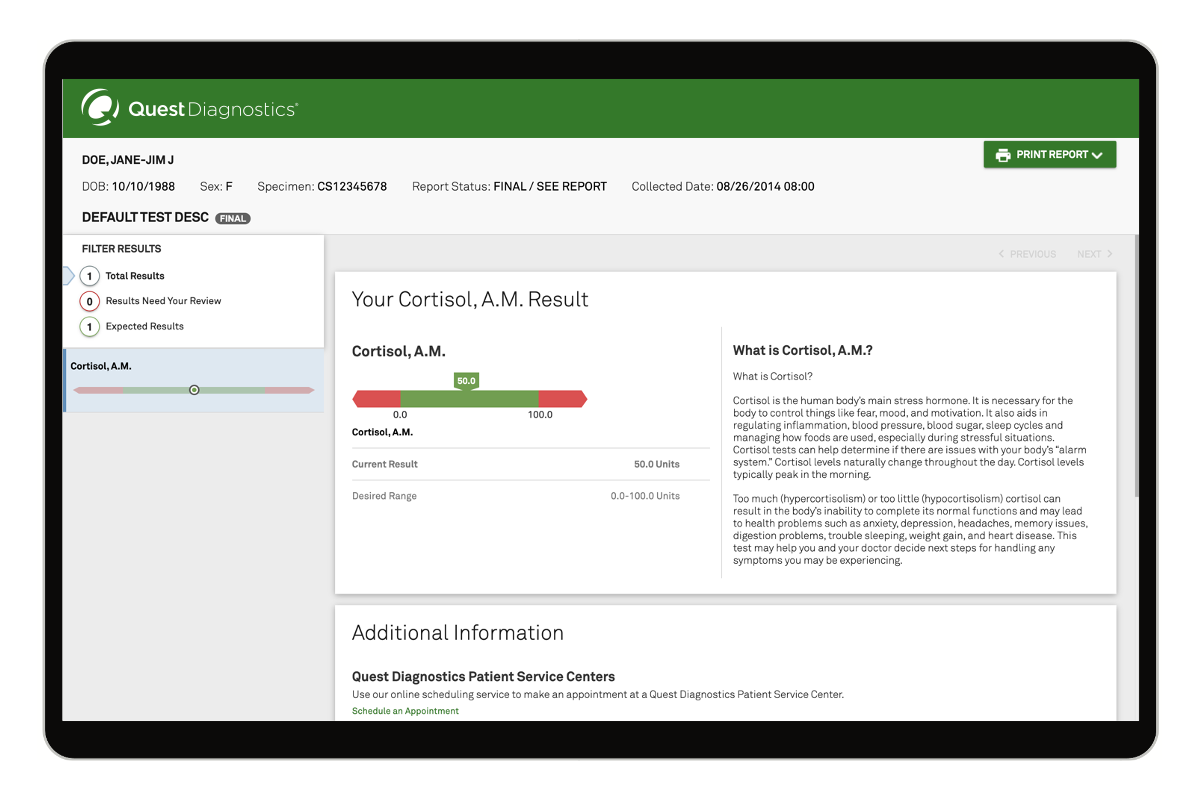
| Cortisol (AM) | May be low | Check for broader hypopituitarism. |
Sometimes doctors run a TRH stimulation testinjecting thyrotropinreleasing hormone and watching TSH rise. In pituitary disease, the TSH response is blunted or absent.
Imaging, usually a sellar MRI with contrast, confirms the structural causewhether its a tumor, hemorrhage, or infiltrative change.
Treatment Options
Now, the question youve been waiting for: What can I do? The answer is twofoldreplace the missing hormones and address the underlying cause.
Hormone Replacement
Levothyroxine (synthetic T4) is the cornerstone. The trick is to titrate the dose to keep free T4 in the middle of the reference rangesince TSH is unreliable here. Your endocrinologist will likely check labs every 68 weeks until stable.
Targeting the Root Cause
- Surgery Transsphenoidal removal of adenomas often restores pituitary function, but not always. A postop scan and hormone panel will guide further therapy.
- Radiation For tumors that cant be safely removed, stereotactic radiosurgery (Gamma Knife) can shrink the lesion over months.
- Medical therapy If the tumor is a prolactinoma, dopamine agonists (like cabergoline) can shrink it and improve TSH output.
- Managing infiltrative disease Treat the primary condition (e.g., chelation for hemochromatosis) to halt pituitary damage.
Dont forget that if multiple pituitary axes are low, you may need cortisol replacement firstotherwise levothyroxine can trigger a crisis. This is why a comprehensive endocrine evaluation is vital.
Monitoring & FollowUp
Regular lab checks (free T4, cortisol, sex steroids) and annual MRIs keep you on track. Many patients find a simple symptom diaryrating energy, temperature sensitivity, and moodhelps their doctor finetune doses.
Balancing Benefits & Risks
Any treatment has a tradeoff, and being aware of both sides empowers you to make informed choices.
Benefits
- Restored energy and mood stability.
- Normalization of metabolism, which can improve cholesterol and cardiovascular risk.
- Potential reversal of menstrual or sexual dysfunction.
Risks
- Overreplacement may cause subclinical hyperthyroidismthink palpitations, anxiety, and bone loss over time.
- Surgical complications (CSF leak, hormonal deficits).
- Radiationinduced hypopituitarism years down the line.
Balancing these means close collaboration with an experienced endocrinologist. A skilled clinician will regularly reassess both lab data and how you feel daytoday.
When to Seek Medical Help
Some redflag signs scream call your doctor now:
- Sudden vision changes or double vision (possible tumor growth).
- Severe fatigue accompanied by dizziness or fainting (possible adrenal insufficiency).
- Rapid weight loss despite loss of appetite (could hint at a different endocrine issue).
- Persistent low mood or depression that doesnt improve with standard therapy.
If any of these appear, schedule an appointment ASAP. Bring a list of current medications, a recent symptom log, and, if possible, a copy of any prior imaging or labs. That preparation makes the visit smoother and lets the specialist zero in on what matters.
Conclusion
Pituitary hypothyroidism can feel like a hidden maze because the usual highTSH clue is missing. Yet, once you understand the pituitary hypothyroidism causesfrom tumors and surgery to injury and infiltrative diseaseyou can spot the symptoms, get the right lab work, and pursue targeted treatment that truly lifts the fog.
Remember, the journey is personal. Some days will be better than others, and thats okay. Keep an open line with your healthcare team, track how you feel, and dont hesitate to ask questionsyour voice is a key part of the healing process.
If youve walked this path or are just starting to explore it, know that youre not alone. Knowledge, support, and the right treatment can bring your energy back, one step at a time.
FAQs
What is the main cause of pituitary hypothyroidism?
The most common cause is a noncancerous pituitary tumor (adenoma), which can compress the gland or interfere with hormone production[1][3].
How does pituitary hypothyroidism differ from primary hypothyroidism?
Primary hypothyroidism stems from thyroid gland failure, with high TSH. Pituitary hypothyroidism (secondary) arises from pituitary dysfunction, leading to low or inappropriately normal TSH and low thyroid hormones[1][5].
What are the typical symptoms of pituitary hypothyroidism?
Symptoms include fatigue, cold intolerance, weight gain, dry skin, hair loss, depression, and menstrual irregularities—similar to primary hypothyroidism, but with possible additional pituitary hormone deficiencies[1][3][6].
How is pituitary hypothyroidism diagnosed?
Diagnosis relies on blood tests showing low TSH and low free T4, plus imaging (MRI) to identify pituitary abnormalities[1][5].
What are the treatment options for pituitary hypothyroidism?
Treatment involves thyroid hormone replacement (levothyroxine) and addressing the underlying cause, such as tumor removal or radiation. Regular monitoring and sometimes replacement of other pituitary hormones are needed[1].