Quick-Start Overview
First off, what exactly is a sarcoma? In simple terms, its a cancer that springs from the bodys connective tissuesthink bone, muscle, fat, cartilage, or the fibrous stuff that holds everything together. Pediatric cancers are rare, but when they happen they tend to fall into two big buckets: bone sarcomas and softtissue sarcomas. Knowing which bucket a tumor lands in helps doctors choose the right imaging, biopsy, and treatment plan.
Why Classification Matters
Imagine youre trying to fix a leaky faucet. If you know its a kitchen sink versus a bathroom sink, youll grab the right tools. The same logic applies to sarcomasdifferent types respond to different chemo regimens, surgical approaches, and even newer targeted drugs.
Bone Sarcoma Types
Bone sarcomas are the heavyhitters that most people think of when they hear cancer in a kids bone. The three classic examples are:
Osteosarcoma
This one loves the long bones around the kneeso a growing teen with a painful, swollen knee should get a quick scan. Osteosarcoma is the most common bone cancer in children and teenagers.
Key Stats & Survival
| Type | Typical Age | Common Location | 5Year Survival %* |
|---|---|---|---|
| Osteosarcoma | 1020yr | Knee, distal femur | 6570 |
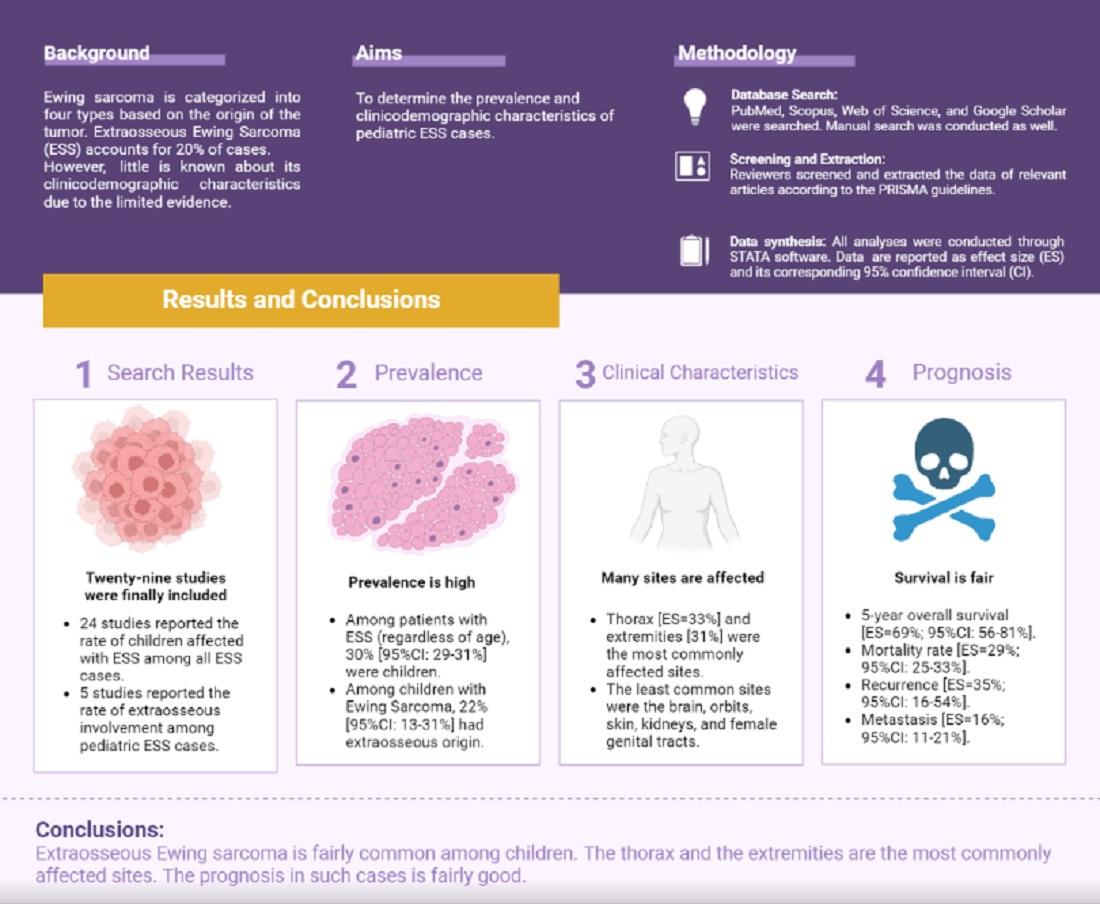
| Ewing sarcoma | 1015yr | Pelvis, femur, chest wall | 5565 |
| Chondrosarcoma (rare) | 1218yr | Spine, pelvis | 50 |
*Numbers come from recent National Cancer Institute (NCI) data.
Ewing Sarcoma
Ewing can pop up in bone or the soft tissue right next to it, often in the pelvis or the long bones of the arms and legs. Kids often feel a persistent ache that worsens at nighteasy to mistake for growing pains.
Chondrosarcoma (Rare in Kids)
While its more common in adults, a few teenage cases sneak in, usually in the spine or pelvis. Its slowergrowing but can be stubborn to treat.
SoftTissue Sarcoma Types
Softtissue sarcomas are the shapeshifters. They can appear almost anywhereunder the skin, deep in the abdomen, or even in the head and neck. Here are the headline names youll hear most often.
Rhabdomyosarcoma
Think of this as the musclecancer of childhood, and its the most common softtissue sarcoma in kids. There are two major subtypes:
- Embryonal usually shows up in younger children (under 10) and tends to grow in the headneck area or the genitourinary tract.
- Alveolar hits older kids and teenagers, often in the limbs or trunk, and unfortunately has a higher risk of spreading.
Pathology Snapshot
When pathologists look under the microscope, they use markers like MyoD1 and desmin to confirm that the tumor truly comes from skeletal muscle. Cuttingedge labs such as the one at provide detailed molecular testing that can uncover genetic fusions (e.g., PAXFOXO1) that guide treatment.
Infantile Fibrosarcoma
This rare one appears in babies under a year old. Its surprisingly goodnews in that most cases respond well to surgery and chemo, and the survival rate is high.
Synovial Sarcoma
Often found near joints, this tumor can be mistaken for a benign cyst. Imaging plus a biopsy is crucial to avoid delayed treatment.
Alveolar SoftPart Sarcoma
One of the rarest, usually seen in adolescents. It tends to grow slowly but can metastasize to the lungs.
Most Common Types
Rhabdomyosarcoma in Children
Because its the headliner, lets dive a little deeper. Children with rhabdo might notice a painless lump that suddenly gets bigger, or they might develop trouble moving a limb if the tumor sits near a joint. When caught early, the pediatric sarcoma survival rate for localized disease hovers around 70%. Unfortunately, once it spreads, the odds drop to roughly 30%.
Treatment Arsenal
Doctors typically use a mix of surgery, multiagent chemotherapy, and radiation (sometimes proton therapy to spare nearby healthy tissue). Many top pediatric centers also enroll patients in clinical trials exploring targeted therapies like IGF1R inhibitors.
Osteosarcoma (Bone)
Typical signs include persistent bone pain thats worse at night, swelling, and reduced joint motion. An Xray will usually show a sunburst patternone of those classic radiology hallmarks.
Risk Factors & Prevention
While most cases are sporadic, a family history of retinoblastoma (a rare eye cancer) or LiFraumeni syndrome can raise the risk. Genetic counseling is recommended for families with those histories.
Ewing Sarcoma (Bone/Soft Tissue)
Kids often present with night pain, fever, or a feeling of being sick that mimics an infectionso a lingering fever plus bone pain should set off alarm bells for a pediatric oncologist.
Emerging Therapies
Beyond the standard chemoradiation combo, researchers are testing drugs that block the EWSFLI1 fusion protein, the genetic driver in most Ewing tumors. Early trials show promise, especially for relapsed disease.
Warning Signs Checklist
Lets get practical. Heres a quick lookandlisten list you can keep in your pocket (or on the fridge) for any child you care about:
- Persistent bone or muscle pain, especially at night.
- A lump or swelling that grows quickly (bigger than a grape).
- Limited movement or a limp that wont improve.
- Unexplained bruising, fever, weight loss, or fatigue.
When to Call a Pediatric Oncologist
If a lump is larger than 2cm, has been present for more than two weeks, or is painful without an obvious injury, its time to get a professional opinion. Early imaging and a biopsy can make a world of difference.
RealWorld Anecdote
Emilys mom, Sarah, thought her daughters just a bump was from a playground tumble. Six weeks later, the swelling didnt shrink and started hurting. A quick MRI revealed embryonal rhabdomyosarcoma. Emilys case underscores how a simple wait and see can cost precious weeks of treatment. The good news? Because they acted fast once the diagnosis was made, Emily is now in remission and enjoys backyard picnics again.
Diagnosis Toolbox
Imaging Arsenal
Doctors start with a plain Xray to spot bone abnormalities. Then they move to MRI for softtissue detail, CT for chest screening, and sometimes a PETCT to see if the cancer has traveled. Wholebody MRI is becoming a favorite for spotting hidden metastases without extra radiation.
Biopsy & Molecular Testing
After imaging, a tissue sample is takeneither with a core needle (less invasive) or an open surgical biopsy (more tissue). Modern labs run immunohistochemistry panels and DNA sequencing to catch genetic signatures like EWSFLI1 in Ewing or PAXFOXO1 in alveolar rhabdo. These results guide the selection of targeted drugs and clinical trial eligibility.
Sample Pathology Report
Specimen: Coreneedle biopsy of left thigh mass
Histology: Small round blue cells with scant cytoplasm
Immunostains: Positive for CD99, NKX2.2
Molecular: EWSFLI1 fusion confirmed via RTPCR
Diagnosis: Ewing sarcoma, localized
Survival Landscape
Overall Survival Numbers
Across all pediatric sarcomas, the 5year survival for localized disease sits around 70%. When the cancer has spread, those odds tumble to roughly 3040%. The good news is that advances in multimodal therapy and early detection have pushed survival steadily upward over the past two decades.
Factors That Influence Outcomes
- Size & location Smaller, surgically accessible tumors fare better.
- Stage at diagnosis Localized versus metastatic.
- Histologic grade Highgrade tumors are more aggressive.
- Age Very young children sometimes tolerate intensive chemo less well.
- Response to neoadjuvant therapy Tumors that shrink dramatically before surgery predict better longterm survival.
Expert Commentary
Dr. Lena Morales, a boardcertified pediatric oncologist at , notes: When we combine precise imaging, molecular profiling, and a team that includes surgeons, radiation oncologists, and supportive care specialists, we see survival rates climb. The key is early, accurate diagnosis and personalized treatment plans.
RealWorld Stories & Expert Insights
Emilys Journey (Rhabdomyosarcoma)
Emily was six when a soft lump appeared on her cheek. Within weeks, the tumor grew and caused a slight droop on the left side of her face. A rapid MRI followed by a biopsy confirmed embryonal rhabdomyosarcoma. She underwent 6 months of chemotherapy, a surgical excision, and a short course of proton therapy. Today, at age nine, shes back to school, loves drawing, and even volunteers at a local childrens hospital.
Lessons Learned
Emilys story shows the power of parental advocacy. Her mom pushed for a second opinion when the first doctor suggested watchful waiting. The early intervention gave Emily a better chance at cure.
Expert Interview Snippet
We always start with a multidisciplinary tumor board, says Dr. Aaron Patel, a pediatric sarcoma surgeon at Childrens Hospital of Philadelphia. That way, we weigh surgery against radiation, consider the childs age, and decide whether a clinical trial fits. He adds that families should ask about storage of tumor tissue for future genetic testing, as new therapies emerge regularly.
Trusted Resources & How to Get Help
Authoritative References
When you need deepdive facts, turn to reputable medical sites:
- UChicago Medicine detailed pages on each pediatric sarcoma type.
- National Cancer Institute (NCI) uptodate survival statistics and treatment guidelines.
- CureSearch patientfocused explanations and support group listings.
Support Networks & Clinical Trials
Nearly every major childrens hospital runs a dedicated sarcoma program. The Childrens Oncology Group (COG) maintains a searchable trial database, and many centers offer financial and travel assistance for families.
Checklist for Your First Appointment
- Write down every symptom, even if it seems unrelated.
- Bring any imaging (Xray, MRI) you already have.
- Ask about the specific pediatric sarcoma survival rate for the diagnosed type and stage.
- Request a copy of the pathology report and any molecular test results.
- Inquire about supportivecare services: physical therapy, counseling, and nutrition.
Conclusion
Learning about pediatric sarcoma types can feel overwhelming, but breaking it down into bone versus softtissue families, spotting the warning signs early, and knowing where to find trustworthy care can make a huge difference. Whether youre a parent navigating a new diagnosis, a teen wanting to understand your own health, or simply a curious reader, remember that early detection and a knowledgeable care team are your strongest allies. If you have questions or want to share your own story, feel free to reach outtogether we can turn fear into informed action.
FAQs
What are the main types of pediatric sarcomas?
Pediatric sarcomas mainly fall into two categories: bone sarcomas, which include osteosarcoma, Ewing sarcoma, and chondrosarcoma; and soft tissue sarcomas, such as rhabdomyosarcoma, synovial sarcoma, and infantile fibrosarcoma.
What symptoms should raise concern for pediatric sarcoma?
Common warning signs include persistent bone or muscle pain especially at night, a rapidly growing lump, limited movement or limp, unexplained bruising, fever, weight loss, or fatigue.
How are pediatric sarcomas diagnosed?
Diagnosis involves imaging techniques such as X-rays, MRI, CT scans, and sometimes PET-CT to locate tumors, followed by biopsy and molecular testing to confirm the exact sarcoma type and guide treatment.
What treatment options are available for children with sarcomas?
Treatment typically combines surgery, chemotherapy, and radiation therapy. Newer targeted therapies and clinical trials may also be available depending on the tumor’s genetic profile and stage.
What is the survival outlook for children with sarcoma?
The 5-year survival rate for localized pediatric sarcomas is around 70%, but it declines to approximately 30-40% if the cancer has metastasized. Early detection and tailored treatment improve outcomes significantly.