Quick answer: If leukemia cells are found in the cerebrospinal fluid, the 5-year survival rate drops dramaticallyabout 11% for AML with CNS involvement and roughly 30% overall, but it jumps to 71% for patients under 15. Knowing these numbers helps you, your loved ones, and your doctors weigh treatment options and plan ahead.
Why it matters: Understanding what leukemia in spinal fluid really means, what symptoms to watch for, and how age shapes prognosis can turn confusion into confidence. Let's walk through everything you need to know, step by step, as if we're chatting over a cup of coffee.
What Does It Mean?
When doctors say leukemia has entered the spinal fluid, they're talking about cancer cells that have leaked into the cerebrospinal fluid (CSF) that bathes the brain and spine. This condition is often called central nervous system (CNS) leukemia or leptomeningeal disease. It isn't a separate disease; it's the same leukemia that's decided to take a detour into the nervous system.
Leukemic cells can reach the CSF in a few ways:
- They travel through the blood and cross the blood-brain barrier.
- They hitch a ride along the nerve roots that extend from the spinal cord.
- In rare cases, they grow directly from the meninges (the protective layers around the brain and spinal cord).
Imagine a tiny, mischievous particle slipping through a crowded hallwayonce it's in the CSF, it can spread quickly, which is why early detection matters.
Survival Statistics
Numbers can feel cold, but they're the most honest way to see the landscape. Below is a snapshot of the most recent data (20232024) from reputable sources such as the National Cancer Institute and peer-reviewed studies.
| Group | 5-Year Survival Rate |
|---|---|
| AML with CSF involvement | 11% |
| Overall AML (any stage) | 30% |
| Children <15 years with AML-CNS | 71% |
| ALL with CNS involvement (children) | 85% |
| Adults 25 years with AML-CNS | 12% |
These figures aren't fate; they're averages. Individual outcomes depend on many factors, which we'll explore next. They remind us, like the survival outlook after prostate removal life expectancy, that treatment success hinges on multiple variables beyond just the diagnosis.
Influencing Factors
Why do some patients beat the odds while others struggle? Here are the main variables that shift the survival curve.
Leukemia Subtype
Acute myeloid leukemia (AML) tends to have a poorer CNS prognosis than acute lymphoblastic leukemia (ALL). The biology of AML cells makes them less responsive to drugs that easily cross the blood-brain barrier.
Timing of CNS Involvement
Finding leukemic blasts in the CSF at diagnosis is usually a better sign than discovering them at relapse, because early, aggressive therapy can be started right away.
CSF Blast Clearance
How quickly the CSF becomes clean after intrathecal chemotherapy is a strong predictor. Studies show that patients whose CSF clears within the first two treatment cycles have a markedly higher survival rate (according to a 2024 ASH Blood article).
Treatment Intensity
Intrathecal chemotherapy, high-dose systemic agents, andin selected caseshematopoietic stem-cell transplant (HSCT) dramatically improve outcomes. However, each comes with its own set of risksagain, age and overall health matter.
Age
Kids are remarkably resilient. The same disease that carries a 12% five-year survival in a 30-year-old may have a 70% chance in a 6-year-old. The reasons include more robust immune systems, better tolerance of intensive therapy, and a higher likelihood of participating in pediatric clinical trials.
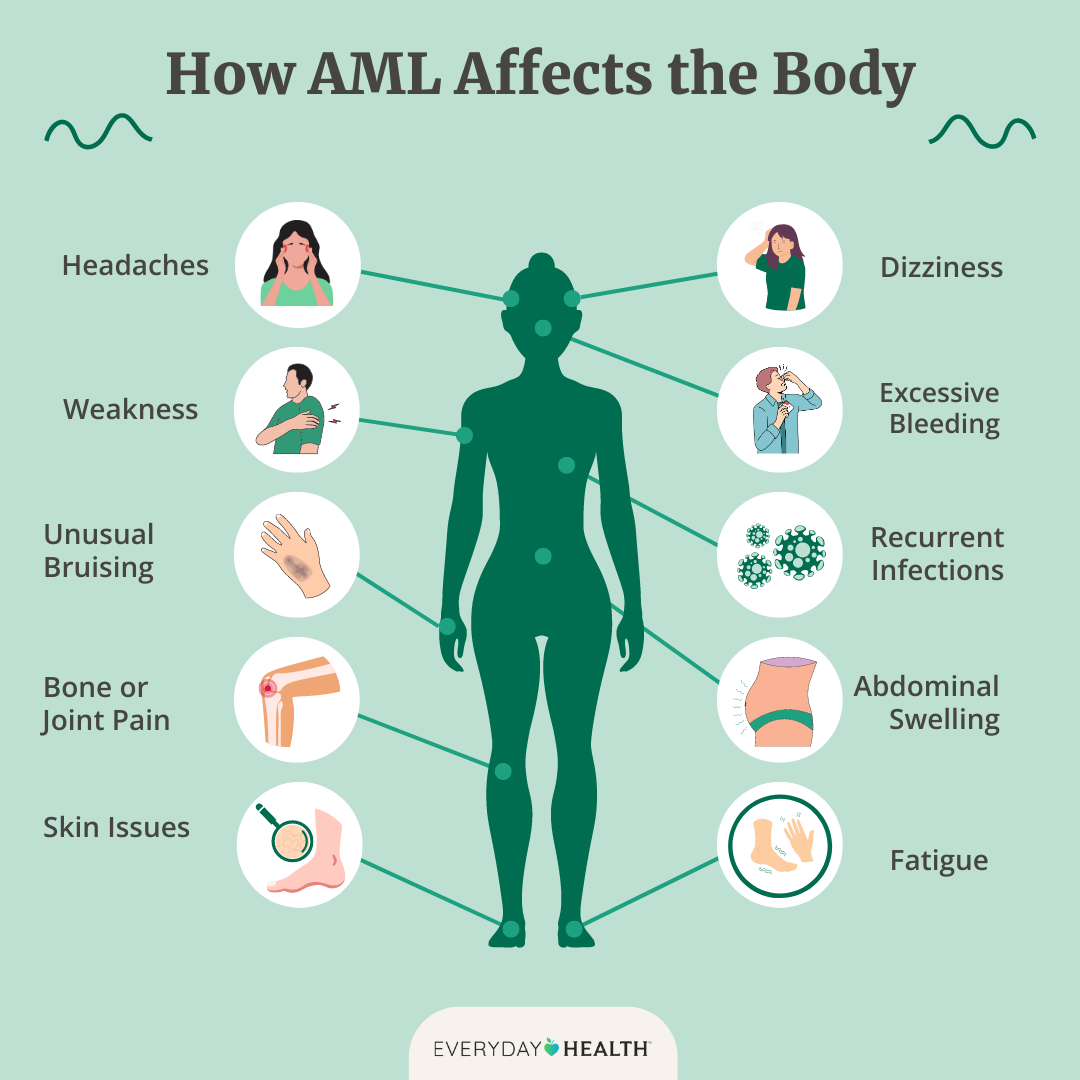
Recognizing Symptoms
When leukemia sneaks into the spinal fluid, it often announces itself with neurological clues. Being alert to these signs can shave weeksor even monthsoff diagnostic delay.
- Headache that worsens when you bend over or lie flat.
- Neck stiffness or a sensation of tightness around the head.
- Photophobia (sensitivity to light) that seems out of proportion.
- Gait disturbancestripping, clumsiness, or feet feel heavy.
- Seizures or sudden changes in consciousness.
For children, the warning signs can look a bit different: persistent irritability, unexplained vomiting, or a new spotty rash on the scalp may be red flags. If you notice any of these, a prompt lumbar puncture can be lifesaving.
How Is It Diagnosed?
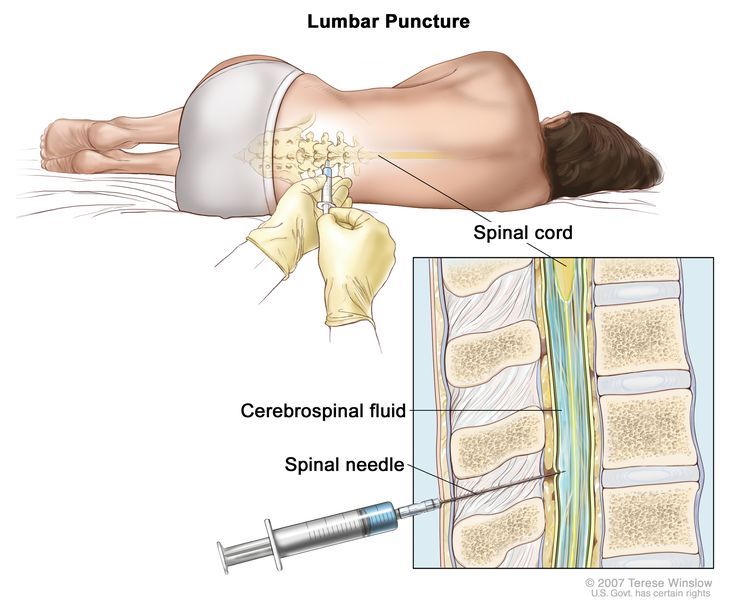
The gold standard is a lumbar puncture, also known as a spinal tap. A small needle is inserted between the lower back vertebrae to withdraw a few milliliters of CSF.
What the Lab Looks For
Laboratories examine the fluid under a microscope for blast cells, run flow cytometry to characterize the cells, and may perform PCR tests for specific genetic mutations.
Imaging Adjuncts
Magnetic resonance imaging (MRI) of the brain and spine can reveal leptomeningeal enhancementbasically, a glow on the images that shows cancer lurking in the membranes. MRI is especially useful when CSF studies are inconclusive.
Combining CSF cytology with flow cytometry increases diagnostic sensitivity from roughly 50% to over 90%, so most modern centers use both methods together.
Treatment Landscape
Knowing the prognosis is only half the battle; the other half is how we fight it. Below is a quick tour of the main weapons in the oncologist's arsenal.
Intrathecal Chemotherapy
Drugs are injected directly into the CSF, bypassing the blood-brain barrier. The classic cocktail includes methotrexate, cytarabine, and hydrocortisone. This approach can achieve CSF blast clearance in 7080% of cases.
Systemic Therapy that Penetrates the CNS
High-dose cytarabine and newer targeted agents like FLT3 inhibitors have shown promise in crossing into the CSF while treating the bulk of the disease.
Cranial/Spinal Irradiation
Radiation can eradicate residual disease but carries long-term riskscognitive decline, growth plate damage in children, and secondary cancers. Modern protocols reserve it for refractory cases or when rapid control is needed.
Hematopoietic Stem-Cell Transplant (HSCT)
For patients whose disease persists after initial therapy, HSCT offers a chance at cure. The transplant replaces the patient's marrow with healthy donor cells, and the high-dose conditioning regimen often wipes out CSF disease as well.
Choosing between these options isn't a one-size-fits-all decision. It requires a multidisciplinary team, the patient's age, overall health, and personal preferencesall weighed together.
Prognosis by Age & Type
Let's pull the numbers together in a way that makes sense for you or someone you care about.
| Age Group | Leukemia Type | 5-Year Survival (CNS Involvement) |
|---|---|---|
| 04 years | AML | 68% |
| 514 years | AML | 71% |
| 1524 years | AML | 38% |
| 25+ years | AML | 12% |
| 014 years | ALL | 85% |
Notice the steep drop after adolescence? It's not just biology; it's also the fact that older patients often receive less intensive CNS-directed therapy because of comorbidities.
If you're reading this as a parent, take heart: children have the best odds, especially when treatment starts early. If you're an adult, the picture looks tougher, but newer targeted drugs and clinical trials are shifting the curve upward.
Resources & Support
Facing leukemia in the spinal fluid is overwhelming, but you don't have to go it alone.
- Leukemia & Lymphoma Society offers financial assistance, education, and connects you with local support groups.
- American Cancer Society provides comprehensive guides and a 24/7 helpline for cancer-related questions.
- HealthTree a patient-run network where families share experiences, treatment tips, and emotional support.
- ClinicalTrials.gov search for ongoing trials targeting CNS leukemia; many are open to pediatric and adult participants alike.
When you feel lost, reaching out to one of these organizations can give you a roadmap, a listening ear, andeven more importantlyhope.
Conclusion
Leukemia in the spinal fluid is a serious development, but it isn't a dead-end sentence. Survival rates vary dramatically with age, leukemia type, and how quickly and aggressively the disease is tackled. Early recognition of symptoms, prompt lumbar puncture, and a tailored combination of intrathecal chemotherapy, systemic drugs, andwhen neededradiation or stem-cell transplant give many patients, especially children, a genuine chance at long-term survival.
Remember, you're not alone on this journey. Talk openly with your medical team, lean on trusted support groups, and stay informed about the latest research. If you have questions or want to share your story, feel free to comment belowyour voice could help someone else find the courage to keep fighting.
FAQs
What does “leukemia in spinal fluid” actually mean?
It refers to cancerous leukemic cells that have entered the cerebrospinal fluid (CSF), the liquid surrounding the brain and spinal cord, a condition called central nervous system (CNS) leukemia.
How does age affect the survival rate for CNS‑involved leukemia?
Children under 15 have dramatically better outcomes (≈ 70 % 5‑year survival) compared with adults, whose survival often falls below 15 %, due to differences in biology and treatment tolerance.
What are the most common symptoms of leukemia in the CSF?
Typical signs include persistent headaches, neck stiffness, photophobia, gait disturbances, and seizures. In kids, irritability, vomiting, or unexplained rashes may also appear.
Which diagnostic tests are used to confirm CNS leukemia?
A lumbar puncture (spinal tap) provides CSF for cytology, flow cytometry, and molecular testing. MRI of the brain/spine can help when CSF results are inconclusive.
What treatment options improve survival when leukemia spreads to the spinal fluid?
Intrathecal chemotherapy, high‑dose systemic agents that cross the blood‑brain barrier, targeted therapies, radiation (in selected cases), and hematopoietic stem‑cell transplant are the main approaches.