But every option comes with its own set of upsides and downsides, so understanding the full picture helps you pick the plan that feels right for your body, budget, and peace of mind.
What Is Osteoporosis
Definition and Risks
Osteoporosis is a condition where the bone tissue becomes porous and fragile, making even a minor fall capable of causing a serious fracture. Think of bone like a honeycomb: when the walls get thin, the whole structure weakens. The biggest danger? Hip, spine, and wrist fractures that can turn a simple stumble into a long, painful recovery.
Lifestyle First
Before you reach for a prescription, most doctors will ask about your daily habits. Calciumrich foods (like dairy, leafy greens, and fortified tofu) and vitaminD (sunlight or supplements) are the building blocks of strong bone. Pair those with weightbearing exerciseswalking, dancing, or light resistance trainingfor about 30 minutes a day, three to four times a week, and youve already laid a solid foundation.
When Medication Becomes Necessary
Lifestyle changes alone work great for earlystage bone loss, but when your bonedensity test (DXA) shows a Tscore of 2.5 or youve already had a fracture, medication steps in. The goal then shifts from prevent loss to actively build back strength.
Key Medication Classes
| Class | Typical Form | Frequency | Key Benefits | Common SideEffects / Safety Concerns |
|---|---|---|---|---|
| Bisphosphonates | Pill or IV infusion | Dailyweeklyyearly | Firstline, costeffective, proven fracture reduction | Stomach irritation, rare atypical femur fracture, jaw osteonecrosis |
| RANKL Inhibitor (Denosumab) | Subcutaneous injection | Every 6months | Strong fracture protection, works when bisphosphonates fail | Skin reactions, rebound bone loss if stopped abruptly |
| HormoneRelated Therapy | Pill/patch | Daily | Helpful for younger postmenopausal women | Bloodclot risk, breastcancer concerns |
| BoneForming Agents | Daily or monthly injection | 112months | Builds new bone, best for severe osteoporosis | High cost, rare osteosarcoma warning |
| SERMs (Raloxifene) | Pill | Daily | Reduces vertebral fractures, protective for breast tissue | Hot flashes, clot risk |
These categories cover the majority of prescriptions youll encounter in 2024. For a deeper dive into each drugs efficacy, offers a clear, researchbacked overview.
Common Treatment Questions
What Is the Best and Safest Treatment for Osteoporosis?
There isnt a onesizefitsall answer, but most experts agree that oral bisphosphonates (like alendronate) are the safest first step for the majority of patients. If you have stomach issues or cant tolerate pills, the injectable denosumab often feels safer because it avoids gastrointestinal irritation.
ProsandCons Snapshot
- Bisphosphonates: Proven track record, inexpensive, but may cause mild heartburn.
- Denosumab: Powerful bone protection, simple injection, but requires a doctors visit every six months.
- Boneforming agents: Build new bone, ideal for severe cases, but pricey and need close monitoring.
How to Treat Osteoporosis Without Medication?
Yes, you can treat the condition through lifestyle aloneespecially if your bone density is only mildly low. Focus on three pillars:
- Nutrition: Aim for 1,200mg of calcium and 8001,000IU of vitaminD daily.
- Exercise: Incorporate weightbearing moves (walking, stair climbing) and resistance work (light dumbbells, resistance bands).
- FallProofing: Keep pathways clear, use nonslip mats, and consider a nightlight to reduce trips.
Regular DXA scans every two years will tell you if these steps are enough or if medication should be added.
What Are the Dangers of Osteoporosis Drugs?
Every medication carries potential risks. With bisphosphonates, the biggest concerns are rare atypical femur fractures and jaw osteonecrosis, especially after longterm use. Denosumabs main warning is a rebound drop in bone density if you stop abruptlyalways plan a transition with your doctor.
Thats why a balanced approachlowdose meds combined with strong lifestyle habitsis often the safest route.
Can Osteoporosis Be Reversed in Six Months?
Shortterm gains are possible, but true reversal in half a year is a stretch. Most studies show measurable bonedensity improvements after 12months of consistent therapy. Think of it like watering a plant: you wont see a full bloom overnight, but youll notice new leaves after a season.
What Is the Best Infusion for Osteoporosis?
If you prefer an infusion over a pill, zoledronic acid (a yearly IV bisphosphonate) and romosozumab (a monthly injection) are the top contenders. Zoledronic acid is affordable and only needed once a year, while romosozumab offers powerful bonebuilding effects but comes with a higher price tag.
I Dont Want to Take Osteoporosis DrugsWhat Are My Options?
That feeling is completely understandable. Many patients start with drugfree strategiesdiet, exercise, and supplementsand keep a close eye on their DXA results. If bone loss continues, a lowdose medication or a shortterm bridge therapy (like a brief bisphosphonate trial) can be a compromise. Always discuss a drug holiday plan with your physician if youre hesitant about longterm use.
Choosing Your Plan
Personal Health Factors
Age, gender, kidney function, and existing gastrointestinal issues all influence which medication works best. For instance, if you have chronic kidney disease, certain bisphosphonates may be off the table, making denosumab a safer pick.
Cost and Access
Generic oral bisphosphonates are usually covered by most insurers, while newer agents like romosozumab might need prior authorization or outofpocket payments. If an infusion center is far from home, a subcutaneous injection you can selfadminister (like denosumab) could save time and travel expenses.
Safety Profile Matching
Match your personal risk tolerance with the drugs safety profile. If youve had stomach ulcers, an injection might be gentler. If youre worried about rare sideeffects like jaw osteonecrosis, a brief trial period with close dental monitoring can help you decide.
Sample Patient Scenarios
- Case A: 58yearold woman, mild GI reflux, recent vertebral fracture. She switched from oral alendronate to denosumab and saw a 7% BMD increase after a year.
- Case B: 72yearold man on chronic steroids, previous bisphosphonate failure. He started monthly romosozumab and stayed fracturefree for 18months.
These stories illustrate how tailoring treatment to individual needs can make a huge difference.
Getting Started Guide
Preparing for Your First Appointment
Bring a list of questions: Whats my fracture risk?, Which sideeffects should I watch for? and How often do I need bonedensity scans? Also, ask your doctor to order baseline labscalcium, vitaminD, and kidney functionto ensure the medication you choose wont cause complications.
Correct Administration Tips
Oral bisphosphonates: Take the pill with a full glass of water first thing in the morning, stay upright for at least 30 minutes, and avoid eating or drinking anything else during that time.
Denosumab injection: Its given under the skin of the upper arm or thigh. Rotate sites each visit and keep the area clean. If you notice any rash or swelling, let your doctor know.
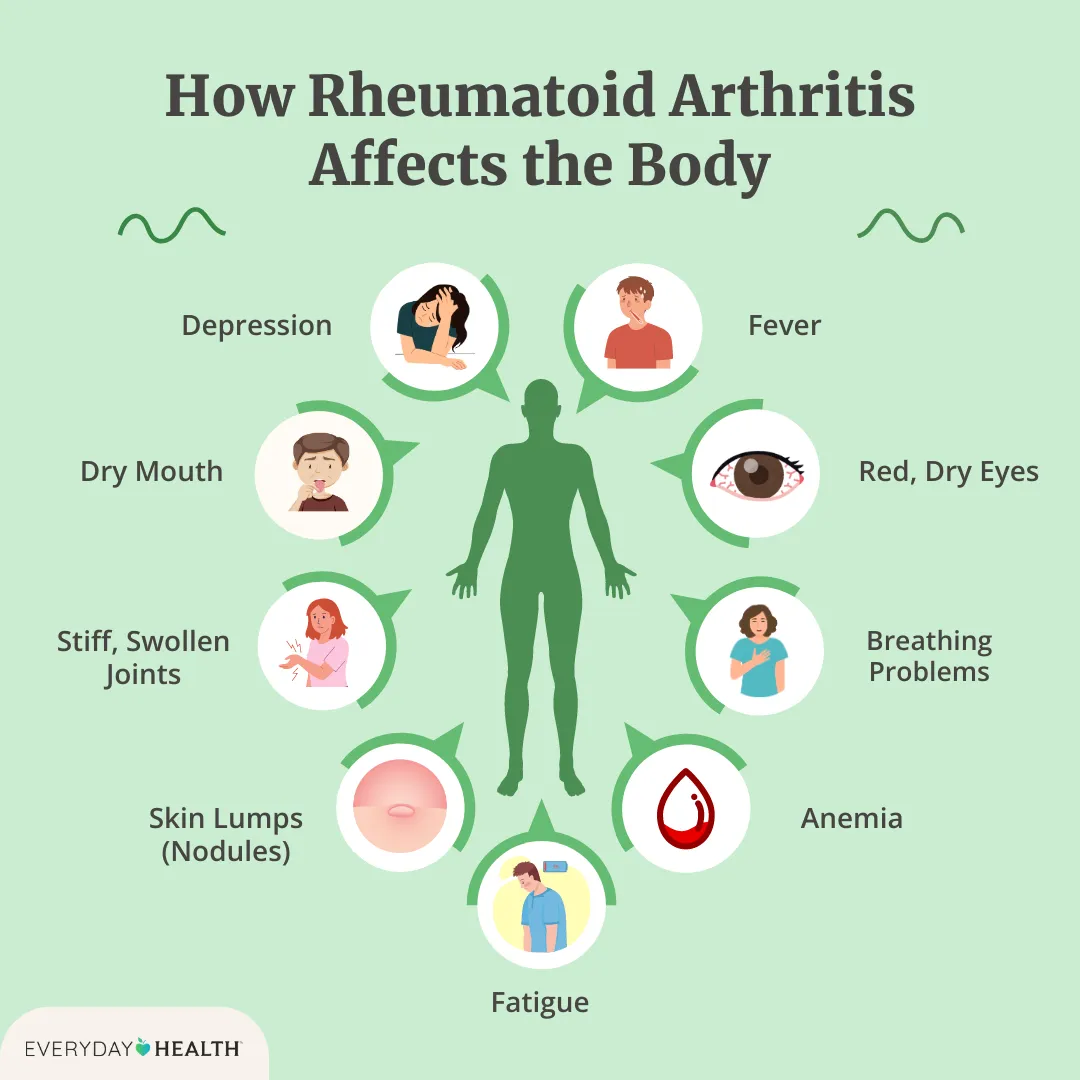
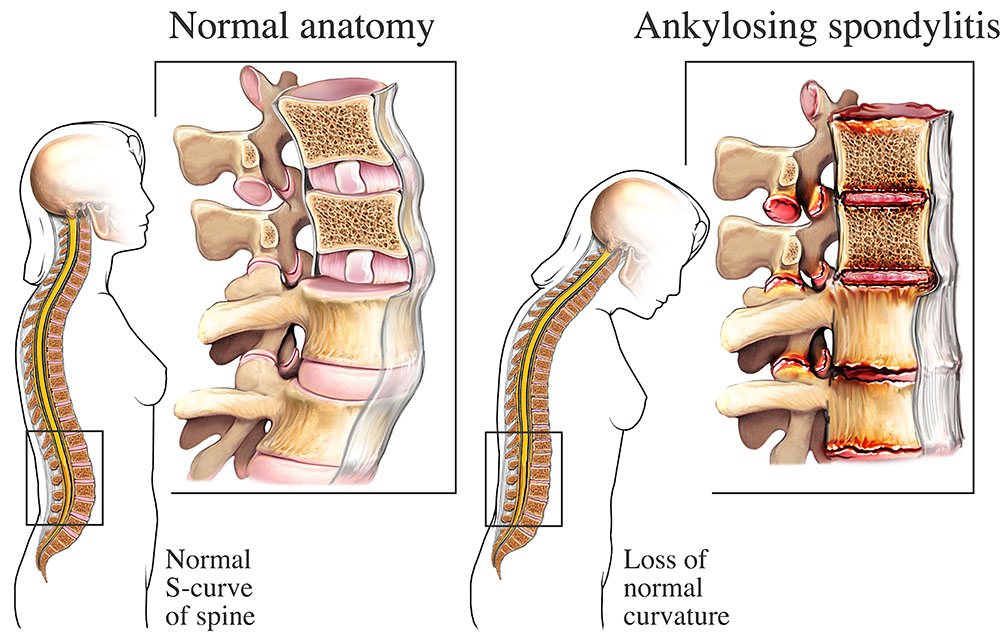
For those managing bone loss along with inflammatory conditions, understanding formal remission definitions can be helpful in coordinating carefor example, clear criteria like ankylosing spondylitis criteria are used in rheumatology to judge disease control and can guide timing of certain osteoporosis treatments when inflammation is also a concern.
Monitoring Progress
Plan a DXA scan every two years to track bonedensity changes. Some doctors also check boneturnover markers (like CTX or P1NP) to see how actively your bone is remodeling. If you notice new thigh or jaw pain, those could be early warning signs.
RedFlag Symptoms
- Sudden, sharp pain in the thigh or groin (possible atypical fracture).
- Unexplained mouth sores, swelling, or jaw pain (look out for osteonecrosis).
- Persistent stomach upset after taking a pill.
Any of these symptoms merit a prompt call to your healthcare provider.
Future Treatment Outlook
Emerging Therapies
Researchers are exploring new drug classes, such as sclerostin inhibitors (like romosozumabs nextgeneration cousins) and selective cathepsinK inhibitors, which aim to boost bone formation while minimizing sideeffects. While promising, these agents are still in clinical trials and wont replace the proven options until they receive full FDA approval.
Staying Informed
Because the field evolves, consider subscribing to reputable newsletters from the National Osteoporosis Foundation or following updates from major endocrinology societies. Staying current ensures youll be ready to discuss the newest evidence with your doctor.
Conclusion
Choosing the right osteoporosis treatment isnt a lottery; its a thoughtful blend of lifestyle habits, medical knowledge, and personal preferences. By understanding the benefits and risks of each optionfrom daily pills to twiceyearly injectionsyou can work with your healthcare team to craft a plan that feels safe, effective, and sustainable. If youve got questions or want to share your own experience, drop a comment below or sign up for our free BoneHealth Checklist to keep track of your progress. Heres to stronger bones and a confident, healthier you!
FAQs
What are the main types of medications used to treat osteoporosis?
The main medication classes include bisphosphonates (oral or IV), RANKL inhibitors like denosumab (subcutaneous injection), hormone-related therapies (pills or patches), bone-forming agents (daily or monthly injections), and selective estrogen receptor modulators (SERMs) such as raloxifene.
Can osteoporosis be managed without medication?
Yes, mild osteoporosis may be managed with lifestyle changes such as calcium and vitamin D intake, weight-bearing exercise, and fall prevention strategies. Regular bone-density monitoring helps assess if medication is needed later.
What are the common side effects of osteoporosis drugs?
Bisphosphonates may cause stomach irritation and rare jaw osteonecrosis; denosumab can cause skin reactions and rebound bone loss if stopped abruptly; hormone therapy carries some clot and cancer risks; bone-forming agents are costly and have rare warnings like osteosarcoma risk.
How often should bone density be monitored during treatment?
Bone density is typically checked with a DXA scan every two years to monitor bone density changes and treatment effectiveness. Some doctors also use bone turnover markers for additional information.
Are there new treatments for osteoporosis on the horizon?
Emerging therapies include sclerostin inhibitors and selective cathepsin K inhibitors that aim to enhance bone formation with fewer side effects. However, these are still in clinical trials and not yet widely available.