How Obesity Drives OA
Mechanical Load: Extra Weight Means Extra Pressure
Every pound you add isnt just sitting on your hips; its multiplied several times across your knees. In fact, a study from the shows that a 10lb weight gain can increase knee joint load by up to 50lb. That extra force speeds up cartilage wear and can turn a minor twinge into chronic pain.
Key Numbers
- Overweight women are about 4times more likely to develop knee OA than women with a healthy weight.
- Overweight men face a 5fold increase in risk.
Inflammation: Fat Tissue Is Not Inert
Beyond the mechanical strain, fat cells secrete inflammatory chemicals called adipokines (think leptin, IL6, TNF). These molecules travel through your bloodstream and amplify the inflammatory storm inside your joints. Thats why people with obesity often see joint pain flare up even in joints that dont bear weight, such as the hands.
How It Works
Leptin, for example, can stimulate chondrocytesthe cells that keep cartilage healthyto produce enzymes that break down that very cartilage. A review in explains this twohit model: mechanical stress plus metabolic inflammation equals accelerated osteoarthritis.
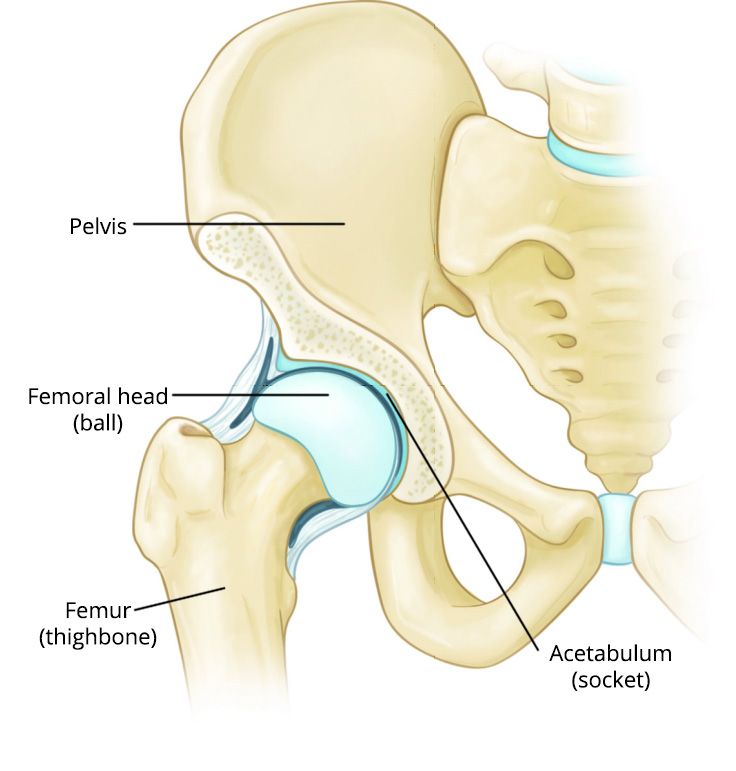
JointSpecific Impact: Knees, Hips, Hands
While the knees feel the most direct hit, obesity also nudges the hips and even the small joints of the hands. The hip joint, for instance, bears the weight of the upper body; a modest 5% loss in body weight can relieve that load enough to cut hip pain by roughly a third, according to recent clinical trials.
Quick Comparison
| Joint | Primary Mechanism | Typical Pain Reduction with 5% Weight Loss |
|---|---|---|
| Knee | Mechanical overload + inflammation | 3040% |
| Hip | Loadbearing stress | 2030% |
| Hand | Systemic inflammation | 1015% |
OA & Obesity Statistics
Global Prevalence and Lifetime Risk
Worldwide, more than 30% of adults are classified as obese, and studies consistently show that obesity roughly doubles the lifetime risk of developing osteoarthritis. A 2024 Nature Review article reported that twothirds of people living with obesity will experience symptomatic knee OA before the age of 70.
BMI Thresholds That Matter
The relationship between bodymass index (BMI) and osteoarthritis is doseresponsive. Heres a quick look:
- BMI 2529.9kg/m (overweight) 1.52 higher knee OA risk.
- BMI30kg/m (obese) 34 higher risk.
- Every 5unit BMI rise adds about a 30% increase in odds of knee OA.
Demographic Nuances
Women tend to develop knee OA earlier than men, possibly because of hormonal influences combined with higher rates of obesity in middle age. Ethnic differences also pop up: in the U.S., AfricanAmerican women have the highest prevalence of obesityrelated knee OA, while Asian populations show a slightly lower risk, likely due to differences in body composition and lifestyle.
Weight Loss and OA
What the Research Says
A systematic review of 15 randomized trials published in 2023 found that a 5% reduction in body weight leads to a 2030% drop in knee pain scores and improves functional performance by about 15%. The same review emphasized that weight loss does not cure osteoarthritiscartilage thats already worn cannot be fully regeneratedbut it can definitely slow further damage and make daily activities easier.
How Much Weight Is Enough?
Even a modest 10lb (4.5kg) loss can trim the knees load by 1550lb. Thats the equivalent of shedding a small backpack of bricks from each knee every step you take.
Practical, EvidenceBased Strategies
Nutrition: Eat to Reduce Inflammation
Adopt a Mediterraneanstyle diet rich in omega3 fatty acids, colorful vegetables, whole grains, and lean protein. A 2022 trial from showed participants who followed this plan lost weight faster and reported lower joint pain than those on a standard lowfat diet.
Exercise: Move Smart, Not Hard
Lowimpact cardiothink brisk walking, water aerobics, or stationary cyclingburns calories without pounding the joints. Pair that with strength training for the quadriceps, hamstrings, and glutes; stronger muscles act as shock absorbers, reducing the stress on cartilage. For targeted rehabilitation, consider exercises used in osteoporosis physical therapy programs that emphasize safe, progressive strengthening and balance work.
Multidisciplinary Programs
Johns Hopkins Joint Health clinic combines physiotherapy, diet counseling, and medical oversight. Patients in their pilot program lost an average of 7% body weight and reported a 35% improvement in pain after six months.
RealWorld Stories & Clinical Insights
Patient Case Study
Sarah, 58, struggled with a BMI of 33kg/m and daily knee pain that kept her from playing with her grandkids. Over a 12month period she trimmed 12kg (26lb) through a mix of Mediterranean meals and twiceweekly water aerobics. Her 6minute walk test jumped from 350m to 460m, and her pain score dropped by 40%a transformation she describes as getting my life back.
Expert Commentary
Dr. Miguel Torres, a boardcertified rheumatologist at Johns Hopkins, says, Weight loss should be the first prescription we give for knee osteoarthritis. Its lowcost, safe, and the benefits stretch far beyond the joints. He adds that patients who combine weight management with targeted physiotherapy see the most lasting results.
Balancing Benefits & Risks
Health Gains Beyond the Joints
Losing weight doesnt just ease your knees; it also lowers blood pressure, improves insulin sensitivity, and lifts mood. Think of it as a winwin: your heart, brain, and joints all cheer you on.
Potential Pitfalls of Rapid Weight Loss
Dropping weight too quickly can lead to muscle loss, which paradoxically puts more strain on your joints. Thats why a steady 0.51kg per week, coupled with protein intake of at least 1.2g per kilogram of body weight, is the sweet spot. Adding resistance exercises helps preserve lean mass while you shed fat.
SafeStep Checklist
- Set realistic goals: 5% weight loss in the first three months.
- Track calories with a reputable app or journal.
- Prioritize protein (lean poultry, fish, legumes).
- Schedule at least 150minutes of lowimpact cardio each week.
- Incorporate two strengthtraining sessions focusing on the legs and core.
- Consult a healthcare professional before starting any new regimen.
Takeaway
Heres the short version: carrying extra weight puts both mechanical pressure and inflammatory fire on your joints, especially the knees, hips, and even the hands. The numbers are clearobesity dramatically raises the odds of osteoarthritis, but the flip side is equally clear: modest, steady weight loss can melt away a good portion of pain, boost mobility, and protect your joints for the long haul.
So, whats next for you? Start with a small, achievable changemaybe swapping soda for water, or adding a 20minute walk after dinner. Talk to your doctor about a tailored weightmanagement plan, and consider joining a community program where you can share experiences and stay motivated.
Wed love to hear your story. Have you noticed a link between weight changes and joint pain? What tricks have helped you stay active? Drop a comment below, and lets keep the conversation going. Together we can turn the tide on osteoarthritis and obesityone step at a time.
FAQs
How does obesity increase the risk of osteoarthritis?
Obesity increases osteoarthritis risk by adding mechanical load to joints, especially knees and hips, and through inflammatory chemicals secreted by fat tissue that damage cartilage.
Can weight loss improve osteoarthritis symptoms?
Yes, losing as little as 5% of body weight can reduce knee pain by 20-30% and improve joint function, slowing further cartilage damage.
What joints are most affected by obesity-related osteoarthritis?
The knees are most affected due to extra mechanical stress, but hips and even hand joints can experience osteoarthritis driven by systemic inflammation.
Is the risk of osteoarthritis the same for men and women with obesity?
No, overweight women have about 4 times the risk of knee osteoarthritis, while overweight men face roughly a 5-fold risk, with hormonal and body composition factors playing a role.
What are safe weight loss strategies to reduce osteoarthritis impact?
Gradual weight loss of 0.5–1 kg per week combining a Mediterranean-style anti-inflammatory diet, low-impact cardio, and strength training is recommended to protect joints and retain muscle.