Hey there, I know the phrase secondary AML can feel like a cold wind on a warm dayunexpected and a bit unsettling. Lets cut through the jargon together and give you the straightup, compassionate rundown you deserve. Below youll find what secondary AML actually means, why it matters, how it shows up, and what the latest treatments and survival numbers look like. Grab a cup of tea, and lets dive in.
What Is Secondary AML?
Plainlanguage definition
Secondary acute myeloid leukemia (secondary AML or sAML) is a type of blood cancer that develops after another blood disordersuch as myelodysplastic syndrome (MDS) or myeloproliferative neoplasm (MPN)or after exposure to chemotherapy or radiation for a different cancer. In short, its not denovo AML that appears out of nowhere; its AML that follows a previous medical event.
How experts label it
Guidelines from the American Society of Hematology (ASH) and the WHO 2022 classification both use the term secondary AML to differentiate it from denovo AML. This distinction matters because it influences risk assessment, treatment choices, and prognosis. According to , secondary AML often carries distinct genetic mutations and a tougher clinical course.
Quicklook comparison
| Feature | Denovo AML | Secondary AML |
|---|---|---|
| Typical onset | Sudden, no prior disease | After MDS, MPN, or chemo/radiation |
| Common mutations | FLT3, NPM1 | TP53, RUNX1, complex karyotype |
| Survival outlook | Higher 5year OS | Lower 5year OS |
Causes & Risk Factors
Therapyrelated AML (tAML)
When a person receives alkylating agents (like cyclophosphamide) or topoisomerase II inhibitors (like etoposide) for another cancer, the DNA in their stem cells can get damaged. Years lateroften 510 yearsthat damage may surface as secondary AML. Radiation therapy can also spark the same problem, especially when large fields are treated.
AML from prior myeloid disease
Patients with MDS, MPN, or even aplastic anemia walk a tightrope. Their bone marrow already struggles to produce healthy blood cells, and a few extra genetic hits can tip the balance into fullblown AML. This pathway is often referred to as secondary AML from MDS. Studies show that about 3040% of MDS patients eventually progress to sAML.
Genetic predispositions
Inherited mutationslike those in TP53, RUNX1, or CEBPAraise the odds of developing secondary AML after an initial insult. Families with a history of myeloid malignancies should consider genetic counseling; early detection can change the game.
Top 5 antecedent disorders
- Myelodysplastic syndrome (MDS)
- Myeloproliferative neoplasm (MPN)
- Previous exposure to alkylating chemotherapy
- Topoisomerase II inhibitor therapy
- Radiation for solid tumors
Symptoms to Watch
Core signs of secondary AML
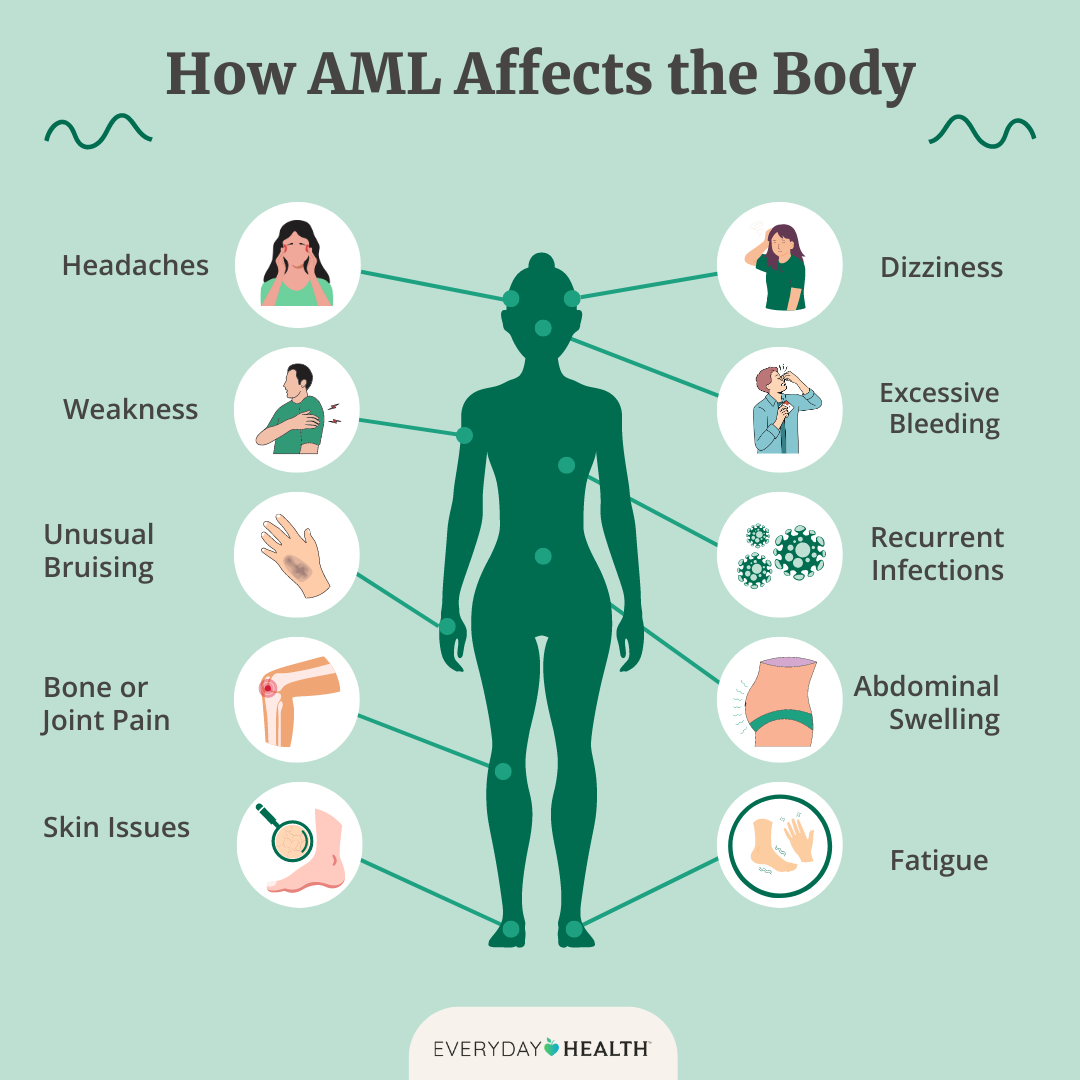
Because secondary AML often emerges in patients already dealing with fatigue, bruising, or anemia from a prior condition, the new symptoms can feel like an echo of the old ones. Keep an eye out for:
- Sudden, worsening fatigue or weakness
- Easy bruising or petechiae (tiny red spots)
- Unexplained fevers or night sweats
- Shortness of breath even with mild activity
- Bone pain, especially in the ribs or long bones
Why they can be masked
If youve been living with MDS, you might already notice low blood counts. Thats why a sharp drop in hemoglobin or plateletsbeyond what youre used toshould raise a red flag. The difference can be subtle, but its a crucial clue for your doctor.
Redflag signs demanding immediate attention
Sudden sharp chest pain, severe bleeding (like nosebleeds that wont stop), or a rapid rise in temperature with no infection source should prompt an urgent medical visit. These could signal the marrows failure to produce enough healthy cells.
Diagnosis & Coding
Laboratory workup
The first step is a complete blood count (CBC) showing blasts (immature cells) over 20% of the white blood cell population. A bonemarrow biopsy follows, giving doctors a look at cellularity, blast percentage, and genetic abnormalities.
Imaging and molecular panels
While imaging isnt usually required to confirm AML, a chest Xray or CT may be ordered to assess for infections or organ infiltration. Molecular testinglike nextgeneration sequencingidentifies mutations such as TP53 or FLT3, guiding targeted therapy decisions.
ICD10 coding for secondary AML
In the International Classification of Diseases (ICD10), secondary AML falls under the C92 series (e.g., C92.0 for AML, not otherwise specified). To denote a secondary origin, clinicians add a secondary diagnosis code that references the antecedent condition (e.g., D46.9 for unspecified MDS). Accurate coding ensures proper billing and epidemiologic tracking.
Example coding table
| Code | Description | When to Use |
|---|---|---|
| C92.0 | Acute myeloid leukemia, not otherwise specified | Primary diagnosis of AML |
| D46.9 | Myelodysplastic syndrome, unspecified | Underlying disease that led to sAML |
| Z85.3 | Personal history of malignant neoplasm of other sites | History of prior solidtumor treatment |
Treatment Options Today
Standard induction regimens
Most patients start with a 7+3 protocol: 7 days of continuous cytarabine infusion plus 3 days of an anthracycline (usually daunorubicin). For older or frail patients, lowdose cytarabine or hypomethylating agents (like azacitidine) may be preferable.
Targeted therapies for secondary AML
When the tumor harbors specific mutations, we have weapons that zero in on them:
- FLT3 inhibitors (midostaurin, gilteritinib) for FLT3mutated sAML.
- IDH inhibitors (ivosidenib for IDH1, enasidenib for IDH2) when those mutations are present.
- BCL2 inhibitor (venetoclax) combined with hypomethylating agentsthis combo has reshaped outcomes for many unfit patients.
Allogeneic stemcell transplant (alloSCT)
If youre a good candidategenerally younger than 70 and with adequate organ functionan alloSCT offers the best chance at longterm remission. The transplant replaces your diseased marrow with healthy donor cells, essentially rebooting the bloodforming system.
Clinicaltrial access & emerging agents
Because secondary AML historically carries a poorer prognosis, many centers encourage enrollment in trials evaluating novel agents like menin inhibitors or antibodydrug conjugates. Always ask your hematologist about available studies; they can sometimes be the key to cuttingedge care.
Prognosis & Survival
Overall survival statistics
Data from large registries indicate a 5year overall survival (OS) of roughly 1020% for secondary AML, compared with 3040% for denovo AML. The exact secondary AML survival rate hinges on age, cytogenetics, and response to induction therapy. For patients concerned about life expectancy related to cancer treatments, it may be helpful to understand prostate removal life expectancy as an example of survival outcomes in cancer care, which you can read more about here.
Factors influencing outlook
- Age Younger patients (<60) fare better.
- Genetic profile TP53 mutations are associated with the lowest survival.
- Prior disease sAML arising from MDS often has a slightly better outlook than therapyrelated AML, though both are challenging.
- Treatment intensity Those who can undergo transplant have substantially higher longterm survival.
Visual survival guide
Imagine a bar graph where the blue bar (therapyrelated AML) sits at about 12% 2year survival, while the orange bar (MDSderived sAML) reaches roughly 20%. This visual helps put raw numbers into perspective and shows the incremental benefit of newer therapies.
Living With sAML
Managing side effects & supportive care
Even the most advanced treatments can bring fatigue, infections, or low blood counts. Here are some practical tips:
- Stay hydrated and prioritize proteinrich meals to support marrow recovery.
- Schedule regular transfusions if anemia or thrombocytopenia become problematic.
- Use prophylactic antibiotics or antifungals as prescribedprevention is better than cure.
Psychological impact & coping strategies
Its normal to feel a swirl of emotionsanger, fear, hopeall at once. Connecting with a support grouplike those run by the Leukemia & Lymphoma Societycan provide a safe space to share and learn. Mindfulness, gentle yoga, or even short daily walks can help anchor you amid the storm.
Practical resources
When youre overwhelmed, having a checklist can bring order:
- Bring a list of current medications to every appointment.
- Ask about the latest clinical trialsask, Are there any ongoing studies that might be right for me?
- Keep a symptom diary (date, severity, triggers) to spot patterns.
- Know your insurance coverage for transplant, targeted drugs, and supportive care.
Personal story snippet
Maria, a 58yearold former chemopatient, shared that learning her sAML was therapyrelated initially felt like a punch. But once her team explained the role of venetoclax plus azacitidine, she felt a flicker of hope. Today, shes in remission and volunteers to mentor newly diagnosed patients, proving that knowledge truly empowers.
Conclusion
Understanding the secondary AML definition isnt just an academic exercise; its the first step toward navigating a complex diagnosis with confidence. You now know why its called secondary, what triggers it, how it presents, and the modern tools doctors use to fight it. Survival rates remain modest, yet advances in targeted therapy and transplant are shifting the landscape brighter each year.
If you or a loved one are facing this journey, remember youre not alone. Arm yourself with the facts, ask pointed questions at each appointment, and lean on the community of patients, advocates, and specialists who genuinely care. Together, we can turn uncertainty into informed actionand maybe, just maybe, a better tomorrow.
FAQs
What exactly is a secondary AML definition?
Secondary AML (sAML) is acute myeloid leukemia that occurs after a prior myeloid disorder (like MDS or MPN) or after exposure to chemotherapy or radiation.
Which factors most commonly cause secondary AML?
Therapy‑related exposure to alkylating agents or topoisomerase II inhibitors, prior myelodysplastic syndrome or myeloproliferative neoplasm, radiation therapy, and inherited mutations such as TP53 or RUNX1.
How do the symptoms of secondary AML differ from its predecessor disease?
Symptoms often mirror those of the earlier disorder but appear suddenly or worsen—new severe fatigue, rapid drop in blood counts, easy bruising, fevers, and bone pain are key warning signs.
What are the main treatment options for secondary AML today?
Standard 7+3 induction, hypomethylating agents plus venetoclax, targeted drugs for FLT3, IDH1/2, or BCL‑2 mutations, and allogeneic stem‑cell transplant for eligible patients.
What is the current prognosis for patients with secondary AML?
Overall 5‑year survival is roughly 10‑20%, lower than de‑novo AML; prognosis improves with younger age, favorable genetics, and successful transplant.