If youve ever felt food stuck before it reaches your throat or noticed yourself coughing every time you take a bite, you might be experiencing oropharyngeal dysphagia. Its a swallowing problem that starts in the mouth or the upper throat, and it can turn everyday meals into a stressful ordeal.
Below youll find a friendly, downtoearth guide that breaks down why this happens, what to look out for, and how modern treatments can help you get back to enjoying food againno medical jargon, just clear answers you can use right now.
Understanding Oropharyngeal Dysphagia
What the term really means
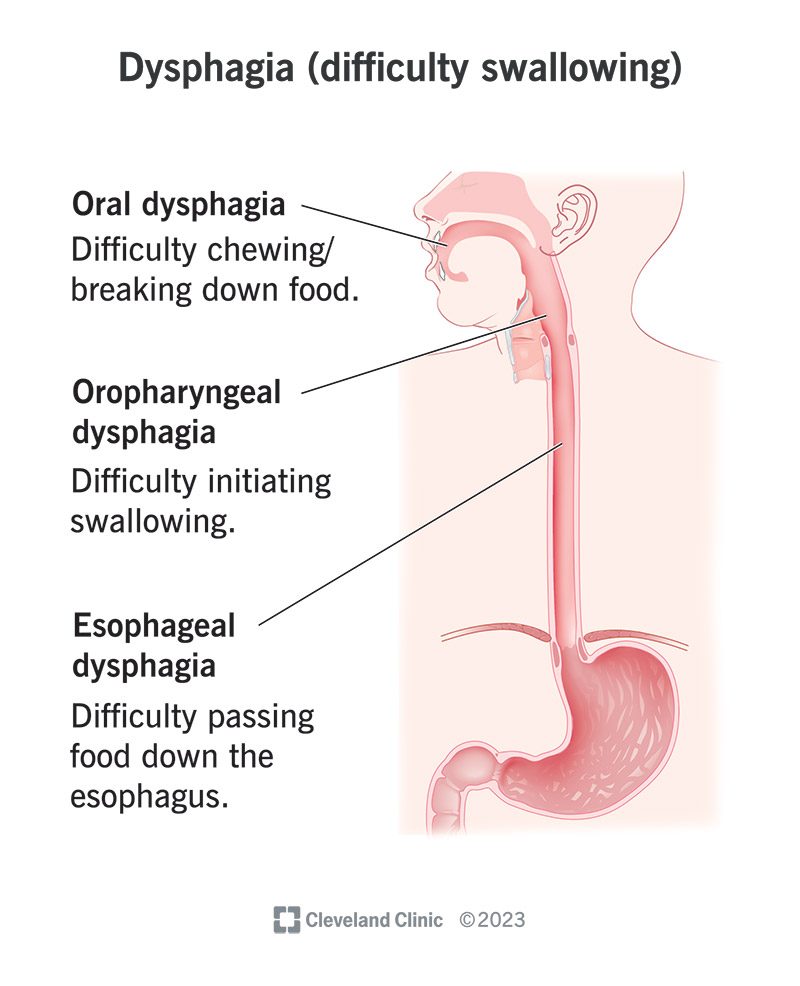
Oropharyngeal refers to the mouth (oro) and the part of the throat right behind it (pharynx). Dysphagia simply means difficulty swallowing. Put together, the phrase describes trouble getting food or liquid out of the mouth and into the esophagus.
How it differs from esophageal dysphagia
While oropharyngeal dysphagia affects the first stage of swallowing, esophageal dysphagia occurs further down, where the food travels through the tube (esophagus) to your stomach. The two can feel similar, but the underlying causes and tests are often quite different.
| Feature | Oropharyngeal Dysphagia | Esophageal Dysphagia |
|---|---|---|
| Location | Mouth & upper throat | Lower throat & esophagus |
| Typical Symptoms | Difficulty initiating swallow, coughing, choking | Feeling of blockage midchest, heartburn |
| Common Causes | Neurologic or muscular problems | Strictures, rings, cancer |
| Key Tests | VFSS, FEES | Endoscopy, barium swallow |
Why the distinction matters
Knowing which part of the swallowing pathway is affected guides the doctor to the right tests and, ultimately, the right treatment plan. Misidentifying the type can lead to unnecessary procedures or delayed care.
Common Causes & Risks
Neurologic conditions
Strokes are the single biggest culpritdamage to the brains swallowing centers can disrupt the coordinated muscles needed to move food forward. Parkinsons disease, multiple sclerosis, and amyotrophic lateral sclerosis (ALS) also mess with the nerves that control the throat.
Muscular disorders
Myasthenia gravis and muscular dystrophy weaken the muscles that open the airway and push food down, making the act of swallowing feel like pushing a boulder uphill.
Structural issues
Tumors, scar tissue from radiation, or even a misaligned jaw can create a physical barrier. In older adults, agerelated muscle atrophy and reduced saliva production add another layer of difficulty.
What is the most common cause?
According to a large epidemiologic study, stroke accounts for roughly 3040% of adult cases of oropharyngeal dysphagia, making it the leading cause.
Risk factors you can watch
Age over 65, a history of head/neck surgery, chronic alcohol use, and certain medications (like anticholinergics) all increase your odds.
Spotting the Symptoms
Core warning signs
- Difficulty starting a swallow (you feel like the food is stuck right at the back of your mouth).
- Frequent coughing or choking during meals.
- Wet or gurgly voice after eating.
- Drooling or excess saliva.
- Unexplained weight loss or recurrent pneumonia.
When the symptoms become urgent
If you notice sudden difficulty breathing, blackouts after swallowing, or a fever that wont go away, call emergency services. Those could signal aspiration pneumoniaa serious complication of dysphagia.
Pronunciation tip
Want to sound confident at your next doctors appointment? Oropharyngeal dysphagia is pronounced oruhfuhRINjeeuhl disFAgeeuh. Feel free to practice in the mirror; the more comfortable you sound, the more likely youll remember to ask the right questions.
How Its Diagnosed
Bedside evaluation
First, a clinician will watch you swallow water and examine the movement of your lips, tongue, and throat muscles. Simple water swallow tests can spot obvious trouble.
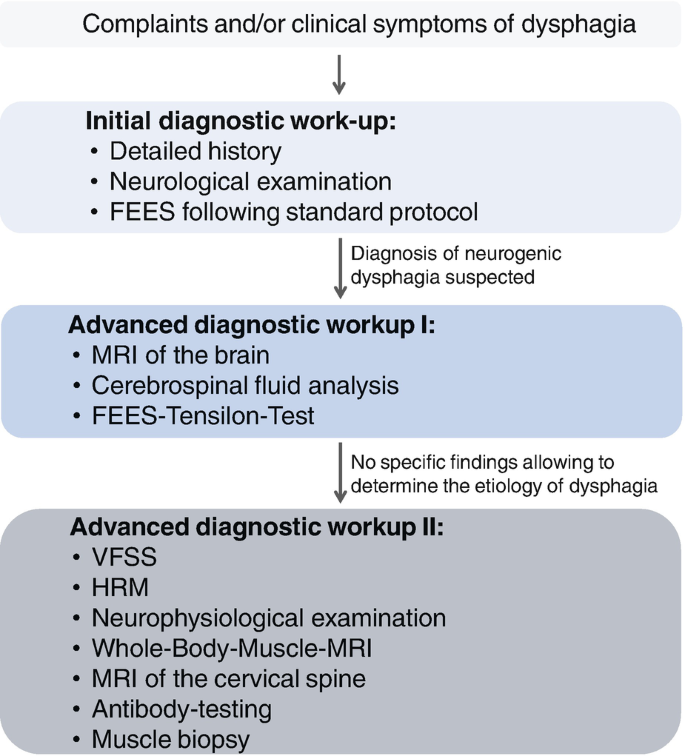
Instrumental studies
Two goldstandard tests are widely used:
- Videofluoroscopic Swallow Study (VFSS) a realtime Xray that shows how food moves through your mouth and throat.
- Fiberoptic Endoscopic Evaluation of Swallowing (FEES) a tiny camera on a flexible tube that lets the doctor see the throat from the inside.
ICD10 coding
When doctors document the condition, they use the code Oropharyngeal dysphagia. Accurate coding helps insurers process claims and researchers track prevalence.
Treatment Options Overview
Rehabilitation therapies
Speechlanguage pathologists (SLPs) design personalized exercise programs. Techniques like the Mendelsohn maneuver or the Shaker exercise strengthen the muscles that open the upper esophageal sphincter.
Dietary modifications
Changing food textures can dramatically reduce choking risk. Pureed foods, thickened liquids, and smaller bites are often recommended while you work on muscle strength. Nutritionists ensure you still get enough calories and protein.
Medical & surgical interventions
For certain cases, doctors may inject Botox into the cricopharyngeal muscle to relax it, or perform endoscopic dilation to widen a narrowed passage. Tumor removal, when applicable, can be curative.
Can it be cured?
Whether cure is possible depends on the cause. If a stroke heals and you complete therapy, many people regain nearnormal swallowing. In progressive diseases like ALS, the goal shifts to maintaining safety and quality of life rather than a full cure.
Balancing benefits and risks
Every treatment carries tradeoffs. Exercises are lowrisk but require time and consistency. Botox can improve opening of the throat but may cause temporary voice changes. A clear prosandcons list helps you and your care team decide together.
Frequently Asked Questions
How is oropharyngeal dysphagia pronounced?
Its oruhfuhRINjeeuhl disFAgeeuh. Think of orapharyngeal followed by disfageeuh.
Whats the biggest difference between oropharyngeal and esophageal dysphagia?
The former stops food at the mouth or throat; the latter occurs lower down, often feeling like a blockage in the chest.
Can it be cured?
Yes, if the root cause is treatable (e.g., a stroke that recovers). For chronic conditions, therapy can dramatically improve safety and comfort, even if a complete cure isnt realistic.
Which condition most often leads to this problem?
Stroke is the leading cause, followed by neurodegenerative diseases like Parkinsons.
How do I get the correct ICD10 code?
The official code is . Using it ensures proper billing and data tracking.
Patient Stories & Insights
Case study: Poststroke recovery
John, a 62yearold engineer, struggled to swallow after a minor stroke. After eight weeks of daily SLP sessions, including the Shaker exercise, he progressed from thickened liquids to regular coffee without coughing. His story underscores how focused rehab can restore safe eating.
Case study: Parkinsons and diet tweaks
Maria, 71, found that pureed meals and a tailored oralmotor program helped her keep weight stable for years. She now volunteers at a local support group, reminding others that small texture changes can make a huge difference.
Invite you to share
Have you or a loved one faced swallowing challenges? Drop a comment below or send us a story. Hearing real experiences makes the journey less lonely for everyone.
When to Seek Help
Redflag signs
If you notice sudden weight loss, frequent lung infections, or a feeling that food is constantly stuck, schedule an appointment ASAP. Early evaluation prevents complications like aspiration pneumonia.
Finding the right specialist
Look for a certified speechlanguage pathologist, an otolaryngologist (ENT), or a gastroenterologist experienced in dysphagia. Many hospitals have multidisciplinary dysphagia clinics that bring all these experts together.
What to expect at the first visit
Bring a list of your current medications, any recent imaging (CT, MRI), and be ready to discuss your eating habits. The clinician will likely perform a bedside swallow test and may order VFSS or FEES based on what they find.
Wrapping Up and Next Steps
Weve covered the basics: what oropharyngeal dysphagia is, why it happens, how to spot it, and what you can do to get back to enjoying meals without fear. The key takeaway is that early recognition and a teambased approachmixing therapy, diet changes, and, when needed, medical interventionscan make a world of difference.
If any of this resonates with you, dont wait. Talk to your primary care physician or a speechlanguage pathologist today. And remember, youre not alonesharing your story helps others feel seen and builds a community thats stronger together.
For families navigating complex neurological causes, resources on atypical Rett syndrome may provide useful context about atypical presentations and care approaches.
FAQs
What is oropharyngeal dysphagia?
Oropharyngeal dysphagia is difficulty swallowing caused by problems in the mouth or upper throat, often due to neurological or muscular conditions.
What are the main symptoms of oropharyngeal dysphagia?
Common symptoms include trouble starting a swallow, coughing or choking while eating, drooling, and a feeling that food is stuck in the throat.
What causes oropharyngeal dysphagia?
It is most often caused by stroke, Parkinson’s disease, muscular disorders, or structural issues in the throat or mouth.
How is oropharyngeal dysphagia diagnosed?
Doctors use bedside exams, videofluoroscopic swallow studies (VFSS), and fiberoptic endoscopic evaluations (FEES) to diagnose oropharyngeal dysphagia.
Can oropharyngeal dysphagia be treated?
Yes, treatments include swallowing therapy, dietary changes, exercises, and sometimes medical or surgical interventions.