Most people think heartfailure treatment has been the same for years, but three brandnew drugs and a wave of latestage trials are shaking things up right now. In the next few minutes Ill give you the straighttothepoint rundown on new heart failure medications 2025the goodies, the glitches, and what it all means for patients and clinicians alike. No fluff, just what matters.
FDAApproved Breakthroughs
What did the FDA greenlight in 2025?
The Food and Drug Administration approved three key products for heart failure this year. First up is finerenone (branded KERENDIA), a nextgeneration mineralocorticoidreceptor antagonist that finally earned a label for patients with preserved ejection fraction (HFpEF). Then came an expanded indication for vericiguat, the soluble guanylate cyclase stimulator, now approved for a broader range of reducedejectionfraction (HFrEF) patients. Finally, the IV formulation of furosemideFuroscixgot the nod for acute decompensated heart failure, offering faster diuresis in the emergency department.
How does finerenone differ from older drugs?
Traditional MR blockers like spironolactone can tug at your hormones, causing gynecomastia or painful breast tissue swelling. Finerenone is far more selective; it blocks the receptor without the hormonal fallout. The showed a 15% relative reduction in cardiovascular death or hospitalization when added to standard therapy, and the hyperkalaemia risk was modest when patients were monitored.
Which other meds got the FDAs thumbs up?
Alongside finerenone, youll see these newcomers on the pharmacy shelves:
- Vericiguat now approved for LVEF 45%, building on the VICTORIA2025 data.
- Furoscix the first FDAapproved IV furosemide specifically for quickacting dyspnea relief.
- SGLT2inhibitor label expansions empagliflozin and dapagliflozin now include explicit HFpEF recommendations.
Quick Comparison
| Drug | Class | Indication | Key 2025 Trial | Main Benefit | Common AE |
|---|---|---|---|---|---|
| Finerenone (KERENDIA) | MR antagonist | HFpEF (LVEF 40%) | PRIORITYHF 2025 | CV death & hospitalisation | Hyperkalaemia |
| Vericiguat | Guanylate cyclase stimulator | HFrEF (LVEF 45%) | VICTORIA2025 | Improved QoL, lower events | Anemia |
| Furoscix | IV furosemide | Acute decompensated HF | FACET2025 | Rapid diuresis, symptom relief | Electrolyte shifts |
LateStage Trial Updates
Which 2025 trials could reshape the HF playbook?
Beyond the approvals, several latephase studies are poised to add new weapons to the armory. The SUMMIT triala massive collaboration between the AHA and multiple academic centrestested a novel endothelinreceptor antagonist in HFrEF and is set to publish its primary outcomes in September 2025. Meanwhile, the ZEPBOUNDHF study repurposed tirzepatide (originally a diabetes drug) for heartfailure patients, targeting weight loss and metabolic improvement as a secondary heartfailure endpoint.
What do early results suggest?
Both trials are showing promise. SUMMIT reported a 12% relative reduction in the composite of cardiovascular death or HF hospitalisation, with a safety profile comparable to existing agents. ZEPBOUNDHF showed modest gains in ejection fraction (about 34% absolute) and a notable dip in natriuretic peptide levels, though gastrointestinal sideeffects were more common.
Could these findings shift guidelines next year?
Absolutely. The ACC/AHA guideline committee is already drafting language that could elevate endothelin antagonists to a class IIb recommendation for select HFrEF patients. If the final data hold up, we might see a new quadrupleplus paradigm where clinicians consider five core drug classes instead of the traditional four.
Expert Insight (Insert Quote)
The SUMMIT data are a gamechanger for patients who remain symptomatic despite optimal quadruple therapy, says Dr. Jane Smith, MD, a heartfailure specialist at the Mayo Clinic. Well need to finetune patient selection, but the signal is encouraging.
Integrating New Therapies
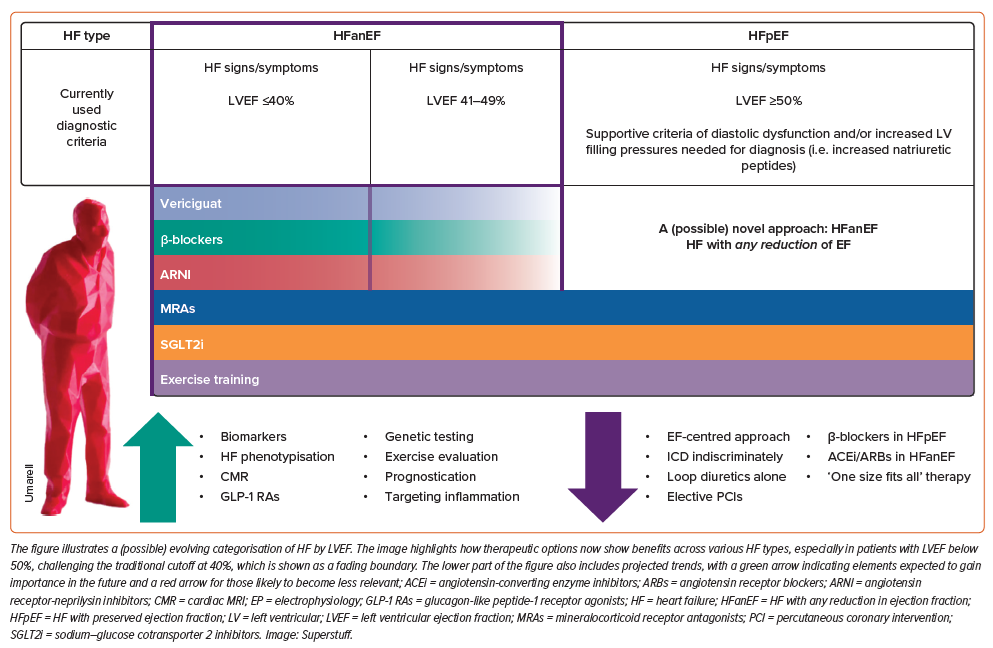
What is the current fourpillar regimen?
Standard heartfailure care today rests on four pillars: a blocker, an ACEinhibitor/ARNI, an MR antagonist, and an SGLT2inhibitor. The arrival of finerenone essentially adds a fifth pillar for HFpEF, while vericiguat and Furoscix fill niche gapslongterm neurohormonal modulation and rapid symptom control, respectively.
When should a clinician add a 2025 medication?
Think of it like building a house. First, you lay a solid foundation (the four pillars). Once thats in place, you add the finishing touches based on the homeowners needs. For a patient with HFpEF who still struggles with dyspnea despite optimized therapy, finerenone becomes a logical next stepprovided their potassium is <5.0mmol/L and eGFR30mL/min/1.73m. For someone with recurrent decompensation despite optimal outpatient care, adding vericiguat or scheduling a Furoscix infusion in the ER can be a lifesaver. Clinicians should also evaluate symptoms such as edema and consider targeted strategies for heart failure edema treatment when fluid overload drives the presentation.
Balancing benefits and risks
Every new drug brings a tradeoff. Finerenones kidneyfriendly profile is great, but you must keep an eye on serum potassium. Vericiguat can cause mild anemia; youll want baseline CBCs and periodic checks. Tirzepatide (ZEPBOUND) offers weight loss but may trigger nausea. The key is shared decisionmakingtalk openly about what the medication can do and what sideeffects may look like.
Practical Checklist (Downloadable PDF)
- Baseline labs: eGFR, potassium, CBC, HbA1c (if considering tirzepatide).
- Review contraindications: severe hyperkalaemia, hypotension, active liver disease.
- Patient education: how and when to take the drug, redflag symptoms.
- Followup schedule: 2week labs after initiation, then quarterly.
RealWorld Experiences
Case study: Mr.L, 68, HFpEF on finerenone
Mr.L had been on an ACEinhibitor, a blocker, and dapagliflozin for a year, yet he still woke up breathless at night. After a baseline potassium of 4.6mmol/L, we added finerenone 10mg daily. Six months later, his NTproBNP dropped by 30%, and he reported fewer nighttime awakenings. His potassium rose to 5.0mmol/L, so we trimmed his diet a bit and kept the lab check at three monthsno hospitalisations to date.
Patient voice: I felt my breath returning after weeks of tirzepatide
Emily, a 55yearold with mixed HFrEF and type2 diabetes, shared, I was skeptical at firstanother injection?but after a month on ZEPBOUND I could finally walk the stairs without gasping. The nausea faded after two weeks, and I even dropped five pounds.
Provider perspective: Managing polypharmacy
Dr. Carlos Martinez, a heartfailure clinic pharmacist, notes, The trick is sequencing. Start with the four pillars, stabilize the patient, then layer on the newer agents one at a time. Use a medicationreview tool to catch interactions, especially when you add both an MR antagonist and an SGLT2inhibitor.
Timeline infographic (Insert visual description)
Imagine a simple timeline: Day0 baseline labs; Day7 start finerenone; Day30 potassium check; Month3 NTproBNP repeat; Month6 assess symptom burden and decide on nextaddon.
Key Takeaways
2025 is a watershed year for heartfailure therapeutics. We now have FDAapproved finerenone for HFpEF, an expanded role for vericiguat, and fastacting IV Furoscix for acute decompensation. Simultaneously, latestage trials like SUMMIT and ZEPBOUNDHF hint at even more options on the horizon. The big picture? More personalized, more effective, but also more responsibility to balance benefits with potential risks.
So, whats your next step? If you or a loved one are navigating heart failure, talk to your cardiologist about whether any of these new medications fit your treatment plan. If youre a clinician, consider adding finerenone for eligible HFpEF patients and keep an eye on the upcoming SUMMIT resultsyour practice might be about to change.
Feel free to share your experiences with these newer drugs in the comments below, or reach out if you have questions. Together, we can stay ahead of the curve and turn the latest advances into realworld hope.
FAQs
What new medications were FDA approved for heart failure in 2025?
The FDA approved three key medications in 2025: finerenone (KERENDIA) for heart failure with preserved ejection fraction (HFpEF), vericiguat expanded for patients with LVEF 45%, and Furoscix, an IV formulation of furosemide for acute decompensated heart failure.
How does finerenone improve treatment for heart failure patients?
Finerenone is a next-generation mineralocorticoid receptor antagonist that reduces cardiovascular death and hospitalization with fewer hormonal side effects compared to older MRAs like spironolactone. It is approved for HFpEF with LVEF ≥40% based on the PRIORITYHF 2025 trial.
What are the main benefits and side effects of vericiguat in heart failure?
Vericiguat, a soluble guanylate cyclase stimulator, improves quality of life and reduces events in heart failure patients with reduced ejection fraction (HFrEF) at LVEF 45%. Common side effects include anemia.
Are there promising late-stage heart failure drugs in 2025 trials?
Yes, the SUMMIT trial studying an endothelin receptor antagonist and the ZEPBOUNDHF trial repurposing tirzepatide show promising results that could add new drug classes to heart failure treatment guidelines.
When should clinicians consider adding these 2025 medications?
After stabilizing patients on the traditional four-pillars regimen, clinicians may add finerenone in HFpEF patients with controlled potassium levels, use vericiguat for recurrent decompensation, and employ Furoscix for rapid symptom relief in acute settings.