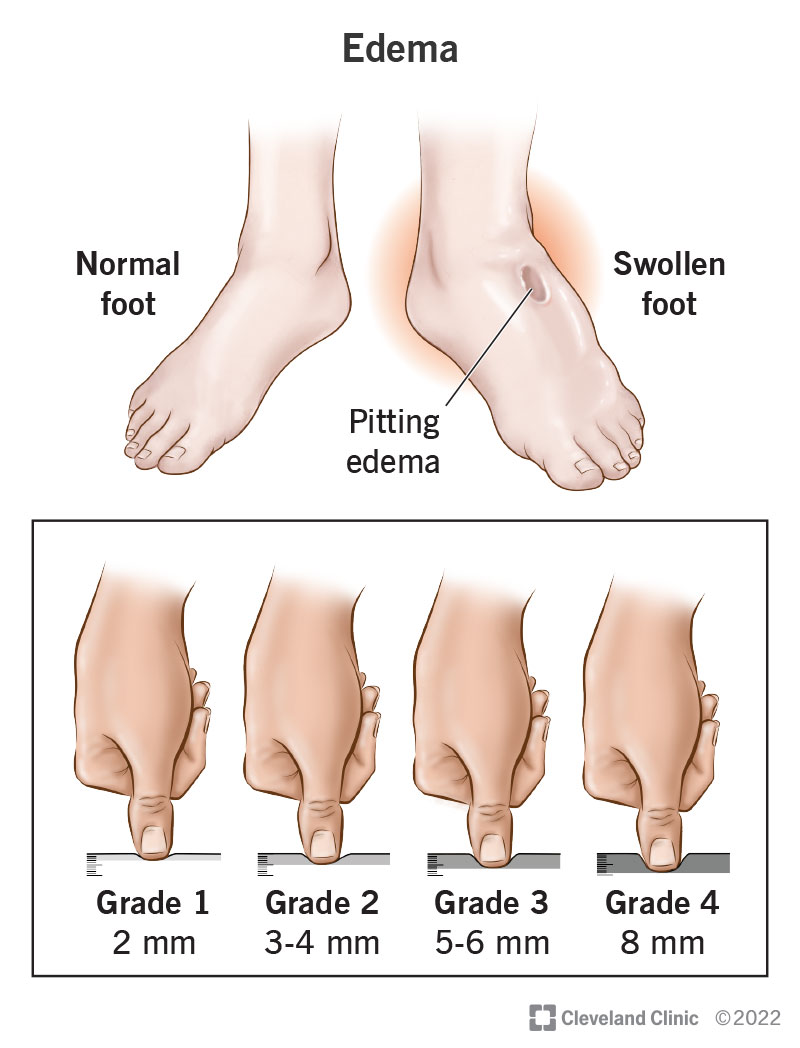
Ever noticed a tiny dent in the skin of your ankle after you press it and wondered why it happens? That little pit is a pretty loud sign that your heart is struggling to keep fluid where it belongs. In heart failure, a cascade of pressures, hormones, and kidney moves push extra fluid into the tissues, creating what doctors call pitting edema. Recognizing this early can mean the difference between a simple adjustment in medication and a hospital stay.
Why It Matters
Understanding the mechanism behind pitting edema does more than satisfy curiosityit equips you to act before swelling turns into shortness of breath, fatigue, or even a lifethreatening crisis. When you know what's happening under the skin, you can talk to your clinician with confidence, tweak lifestyle habits, and keep the pits from getting deeper.
What Is Pitting?
Pitting vs. NonPitting Edema
Think of pitting edema as a sponge that leaves a temporary dent when you press it, while nonpitting edema feels more like a firm, waterlogged mattress that doesn't rebound. The difference lies in the fluid's composition: pitting edema is rich in sodiumwater that slips easily between cells, whereas nonpitting (often seen in lymphedema) contains proteinladen fluid that sticks.
How It Signals Severity
Doctors use the depth of the pit to gauge how badly the heart is failing. A shallow +1 might just be a hint, but a deep +4 often signals advanced congestion and a higher risk of hospitalization. It's a simple visual cue that packs a lot of prognostic punch.
Core Pathways
Elevated Hydrostatic Pressure The Push
When the heart can't pump efficiently, blood backs up in the veins, raising the pressure that pushes fluid out of the vessels and into the interstitium. This is the classic Starling force scenario: higher capillary pressure forces more fluid into the surrounding tissue.
Reduced Oncotic Pressure The Pull
If albumin or other plasma proteins drop (think chronic liver disease or severe malnutrition), the pull that normally draws fluid back into the vessels weakens. The net result? More fluid stays outside, adding to the swelling.
NeuroHormonal Overdrive
The body senses that blood pressure is falling and flips on a series of emergency systems:
- ReninAngiotensinAldosterone System (RAAS) releases aldosterone, telling the kidneys to retain sodium and water.
- Sympathetic Nervous System constricts vessels and raises heart rate, but also nudges the kidneys toward fluid retention.
- Vasopressin (ADH) tells the kidneys to reabsorb water, further swelling the interstitium.
These cascades are meant to protect you in the short term, but in chronic heart failure they become the main culprits behind edema.
Renal SodiumWater Handling
With reduced cardiac output, the kidneys receive less perfusion, interpreting it as dehydration. They respond by holding onto sodium and water, which then drifts into the legs and abdomen. This maladaptive loop is why diuretics are a cornerstone of heart failure edema treatment recommendations.
Capillary Permeability and Inflammation
Inflammatory cytokines (like TNF) can make capillary walls leaky, allowing even more fluid to slip out. Some clinicians even reference a paper for a deeper dive on this point.
Clinical Presentation
Typical Locations
Most people first notice swelling around the ankles and the lower shinthe lowest point when you're standing. As congestion worsens, fluid can collect around the sacrum, the abdomen (ascites), and even the lungs, leading to the classic wet heart failure symptoms.
Grading Pitting Edema
| Grade | Depth of Pit | Typical Weight Gain (kg) |
|---|---|---|
| 0 | No pit | None |
| +1 | Very shallow (<2mm) | 1 |
| +2 | Moderate (24mm) | 12 |
| +3 | Deep (46mm) | 23 |
| +4 | Very deep (>6mm) skin may stay indented | >3 |
Simply press a finger firmly for a few seconds; if a dent remains, you've got a + grade. It's quick, painless, and surprisingly informative.
RedFlag Symptoms
If swelling accompanies sudden weight gain, worsening shortness of breath, orthopnea (needing extra pillows), or a feeling of tightness in the chest, it's time to call your heart team. Those signs often mean fluid is moving into the lungsa far more dangerous situation.
Diagnostic Workup
Physical Exam Pearls
The press and watch technique we just described is a staple. Additionally, checking the jugular venous pressure (JVP) and listening for crackles in the lungs helps confirm systemic congestion.
Lab Markers
BNP or NTproBNP levels rise when the heart stretches, providing a biochemical clue that fluid overload is worsening. Electrolytes, creatinine, and liver function tests round out the picture, especially when you're planning diuretic adjustments.
Imaging
Bedside ultrasound can measure the inferior vena cava (IVC) diametera wider IVC often correlates with higher rightsided pressures. A standard chest Xray shows vascular congestion, while an echocardiogram quantifies ejection fraction and valve function.
When to Use a Edema PDF
Specialist handoffs sometimes request a concise pathophysiology of edema PDF that summarises the mechanisms and treatment plan. Having a readymade, wellcited PDF saves time and ensures everyone is on the same page.
Treatment Strategies
Loop Diuretics First Line
Furosemide and torsemide act fast, pulling sodium and water out through the kidneys. The key is to start low, monitor weight daily, and adjust the dose based on how the pit shrinks (or deepens).
ThiazideType AddOn
If the loop alone isn't enoughoften called diuretic resistanceadding a thiazidetype (like metolazone) can unblock the kidneys' reabsorption pathways and give you that extra fluid push.
NeuroHormonal Blockers
ACE inhibitors, ARBs, ARNIs, betablockers, and mineralocorticoid receptor antagonists (MRAs) don't just protect the heart; they blunt the very hormonal drives that cause edema. Think of them as the behindthescenes crew that prevents the flood from happening in the first place.
Lifestyle Tweaks
- Limit sodium to <2g per day (about a teaspoon).
- Watch fluid intakemost clinicians recommend 1.52L per day, but individual needs vary.
- Elevate legs above heart level for 1520 minutes a few times daily.
- Wear compression stockings only if prescribed (they can worsen swelling in severe rightsided failure).
Advanced Options
When medication and lifestyle aren't enough, options like ultrafiltration (a mechanical way to pull fluid out), SGLT2 inhibitors (which have a mild diuretic effect), or cardiac resynchronisation therapy can be considered. A comparison table helps decide when to move to these nextlevel steps.
| Option | When to Consider | Pros | Cons |
|---|---|---|---|
| Ultrafiltration | Severe diuretic resistance | Rapid fluid removal | Invasive, requires monitoring |
| SGLT2 Inhibitors | HFrEF or HFpEF with CKD | Improves outcomes, modest diuresis | Potential genital infections |
| Cardiac Resynchronisation | EF 35% & wide QRS | Reduces hospitalization | Procedural risk |
Prevention & SelfMonitoring
Daily Weight Log
A gain of just 0.5kg over 24 hours can signal fluid accumulation. Keep a small notebook by the bathroom scale; it's the simplest earlywarning system you have.
Home Grading Checklist
Print a onepage Edema Grading Sheet, press each ankle, and write down the grade. Seeing the numbers rise over a few days makes it easier to call your doctor before things get out of hand.
When to Call the Cardiology Team
Any of the following should prompt a phone call:
- Weight gain >2kg in 3 days.
- Edema grade increases by more than one level.
- New shortness of breath, especially when lying down.
- Rapidly worsening fatigue or swelling in the abdomen.
RealWorld Case Study
Meet Mary
Mary, a 72yearold retired teacher, was diagnosed with heart failure with preserved ejection fraction (HFpEF). Over a winter month, she noticed her ankles swelling to a +3 grade after a short walk. Her weight jumped from 68kg to 71kg, and she felt unusually short of breath climbing a single flight of stairs.
Diagnostic Journey
Her primary care doctor measured her BNP (560pg/mL) and ordered an echocardiogram that confirmed diastolic dysfunction. A bedside ultrasound showed an IVC diameter of 2.5cmsignificantly enlarged.
Treatment Adjustments
Mary's doctor increased her furosemide dose, added metolazone, and started an SGLT2 inhibitor. She also received counseling on a lowsodium diet and began daily leg elevation. Within two weeks, her edema grade fell to +1, and she lost 2kg.
TakeAway Lessons
Mary's story highlights three key points:
- Early selfmonitoring can catch fluid buildup before it overwhelms the lungs.
- Combining loop diuretics with a thiazidetype can overcome resistance.
- Modern therapies like SGLT2 inhibitors provide an extra safety net.
Balancing Benefits & Risks
While diuretics relieve swelling, they can also cause electrolyte imbalances, kidney function dips, and low blood pressure. That's why regular labs and careful dose titration matter. On the flip side, undertreating edema leaves you vulnerable to pulmonary congestion, reduced exercise capacity, and repeated hospital trips.
The sweet spot is a personalized plan that reduces symptoms without compromising safetysomething you and your care team can finetune over time.
Conclusion
In a nutshell, pitting edema in heart failure is the visible result of a pressurepush, hormonepull, and kidneyretain dance that goes awry when the heart can't pump effectively. By spotting the dent, understanding why it's there, and acting swiftlywhether through medication tweaks, lifestyle habits, or advanced therapiesyou can keep the fluid where it belongs and stay on the road to better health. Remember, your own observations are powerful clues; keep an eye on those ankles, track your weight, and don't hesitate to reach out when the pit deepens. Together with your healthcare team, you can turn those pits into a manageable part of life rather than a warning sign.
FAQs
What causes pitting edema in heart failure?
Pitting edema in heart failure is caused by increased hydrostatic pressure from poor heart pumping, neurohormonal activation leading to sodium and water retention, and kidney dysfunction that promotes fluid buildup in tissues.
How does the Renin-Angiotensin-Aldosterone System (RAAS) contribute to edema?
RAAS activation causes the kidneys to retain sodium and water, increasing blood volume and pressure, which pushes fluid into the interstitial space, contributing to pitting edema in heart failure.
Why is decreased oncotic pressure important in edema formation?
Lower plasma protein levels, such as albumin, reduce oncotic pressure, weakening the pull of fluid back into blood vessels, thus allowing more fluid to remain in tissues and cause edema.
How is pitting edema graded clinically?
Pitting edema is graded from 0 to +4 based on the depth and duration of skin indentation when pressed, with higher grades indicating more severe fluid accumulation linked to worsening heart failure.
What treatments help reduce pitting edema in heart failure?
Treatments include loop diuretics to remove excess fluid, neurohormonal blockers to reduce hormonal fluid retention, lifestyle changes like sodium restriction, and advanced therapies such as ultrafiltration or SGLT2 inhibitors.