Metastatic soft tissue sarcoma (stage4 sarcoma) means the cancer that started in muscle, fat or connective tissue has spread to other parts of the bodymost often the lungs, liver or bone. On average, life expectancy ranges from about 12 to 24 months, though many factors can move that number up or down.
Why does this matter? Knowing the warning signs, how doctors confirm the spread, and which treatments are available can give you (or a loved one) a clearer roadmap, help you ask the right questions, and make decisions that feel right for your situation.
Understanding Metastatic Sarcoma
Definition and key differences
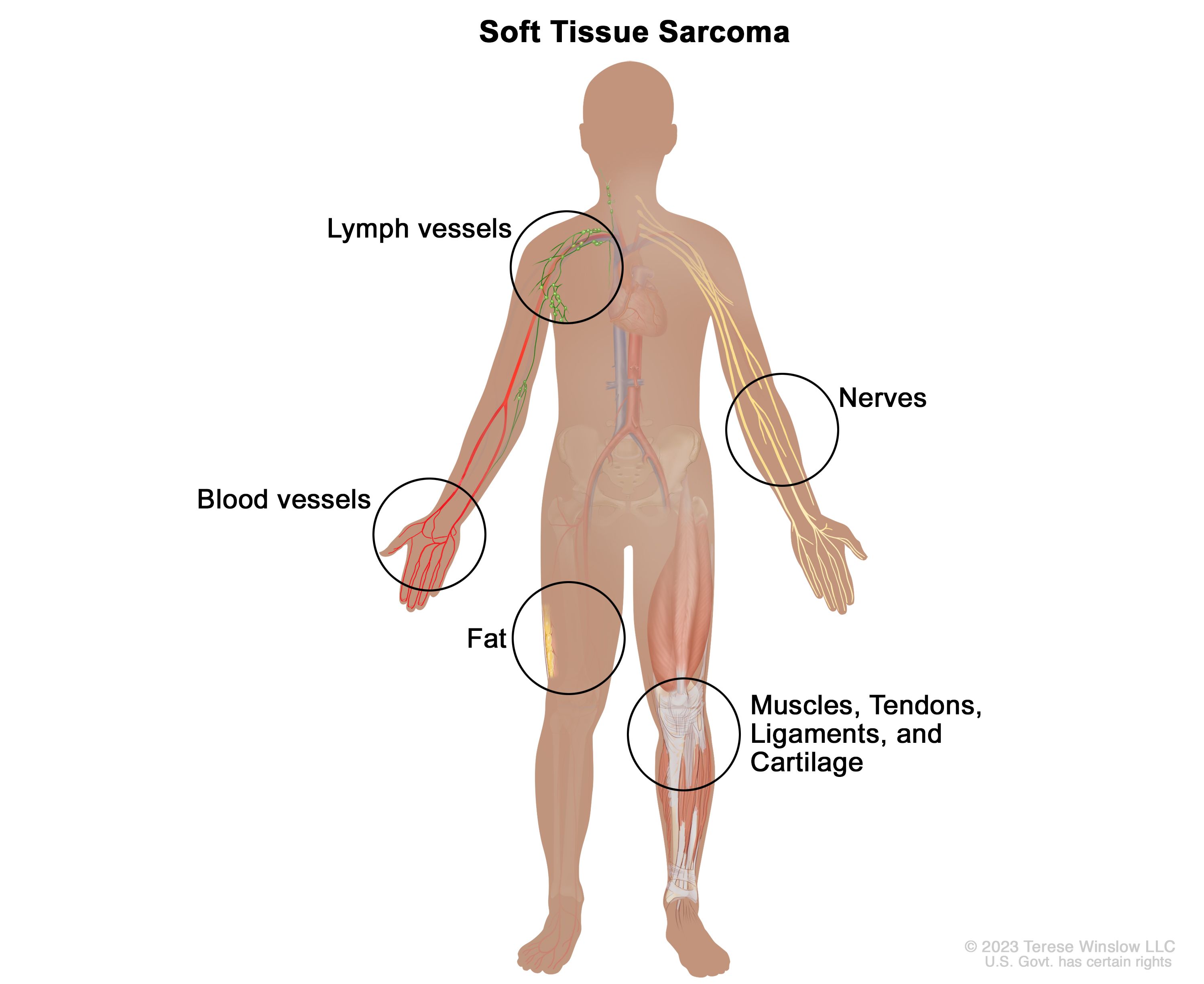
When a soft-tissue sarcoma stays inside its original spot, it's called localized. Once cancer cells break free and travel through blood or lymph vessels to form new tumors elsewhere, the disease becomes metastatic. This shift changes the treatment plan, the prognosis, and often the emotional landscape.
Common subtypes that spread
| Subtype | Primary tissue | Typical metastasis sites |
|---|---|---|
| Undifferentiated pleomorphic sarcoma | Soft tissue of extremities | Lungs, liver, bone |
| Leiomyosarcoma | Uterus, retroperitoneum | Lungs, peritoneum |
| Synovial sarcoma | Near joints | Lungs, mediastinum |
| Myxoid liposarcoma | Deep soft tissue of thigh | Bone, lungs |
These patterns matter because they guide which scans doctors order first and what we should watch for in the months ahead.
Why expertise matters
According to a senior sarcoma oncologist at the , specialized centers see better outcomes because they combine surgical skill, advanced imaging, and clinical-trial access under one roof.
Recognizing the Symptoms
General redflags
Everyone feels off from time to time, but certain changes should raise a louder alarm: persistent pain that doesn't improve with rest, unexplained weight loss, extreme fatigue, or a new lump that keeps growing.
Sitespecific signals
Lung involvement
A cough that lingers, shortness of breath that worsens, or a sharp chest painespecially if you've already had a sarcomaare classic signs that the disease may have spread to the lungs.
Bone involvement
Sharp, localized bone pain, fractures from minimal trauma, or a tingling sensation down a limb often point to bone metastases.
Liver or brain spread
Swelling or discomfort in the upper abdomen, jaundice, headaches, vision changes, or sudden balance problems could signify liver or brain involvement.
When to call your doctor
If any of these symptoms appear together, or if a new symptom seems out of character, pick up the phone. Early detection of a new metastatic site can open up treatment options that might not be available later.
How Diagnosis Works
Imaging workup
Doctors typically start with a high-resolution CT scan of the chest because the lungs are the most common destination. A whole-body PET-CT can then map out any additional hotspots, while MRI excels at visualizing bone and soft-tissue lesions.
Biopsy and pathology
Seeing something on a scan isn't enoughtissue proof is essential. A core needle biopsy, often performed under CT guidance, provides cells that a pathologist can examine for the exact sarcoma subtype and any molecular alterations that might open the door to targeted therapy.
Staging systems
The American Joint Committee on Cancer (AJCC) 8th edition labels metastatic disease as Stage IV. This staging helps doctors compare outcomes across studies and decide whether aggressive curative-intent surgery makes sense.
Quick reference staging chart
| Stage | Extent of disease | Typical treatment focus |
|---|---|---|
| I | Localized, low grade | Surgery & radiation |
| II | Localized, high grade | Surgery + chemo |
| III | Large or unresectable primary | Neoadjuvant therapy |
| IV | Metastatic (any site) | Systemic therapy & local control |
Life Expectancy Outlook
Overall survival statistics
Large registry analyses from the report a median overall survival of 1224 months for Stage IV soft tissue sarcoma, with a 5-year survival hovering around 15%.
Factors that shift the numbers
- Number of metastases: Fewer sites generally mean a longer horizon.
- Location: Lung-only disease often carries a slightly better prognosis than liver or brain spread.
- Histologic grade: Low-grade sarcomas tend to behave less aggressively.
- Performance status: Patients who can stay active usually tolerate treatment better.
- Response to first-line therapy: Tumors that shrink on doxorubicin-based chemo often buy extra months.
Stage4 sarcoma life expectancy quick FAQ
Q: What's the typical life expectancy for stage4 sarcoma?
A: On average 1224 months, but some patients live beyond three years, especially when disease is limited to the lungs and responds to treatment. For patients and families seeking detailed prognostic guidance, reviewing literature on related cancers such as prostate removal life expectancy can sometimes help frame questions about functional recovery and long-term planning in survivorship contexts.
Survival comparison by subtype
| Subtype | Median OS (months) | 5yr Survival % |
|---|---|---|
| Undifferentiated pleomorphic | 16 | 12 |
| Leiomyosarcoma | 18 | 14 |
| Synovial sarcoma | 20 | 16 |
| Myxoid liposarcoma | 22 | 18 |
Available Treatment Options
Firstline systemic therapy
The backbone of treatment remains an anthracyclinemost often doxorubicinsometimes paired with ifosfamide. According to a , this combination yields response rates around 25% but brings additional side-effects like nausea and low blood counts.
Targeted and immunotherapy
Pazopanib, a VEGF receptor inhibitor, is FDA-approved for non-adipocytic soft-tissue sarcoma after chemotherapy failure. Early-phase studies also show promise for checkpoint inhibitors such as nivolumab, especially when combined with ipilimumab, though robust data are still emerging.
Local control strategies
Surgery for isolated metastases
If a single lung nodule or a solitary bone lesion is the only site of spread, surgeons can sometimes remove it with curative intent. Success hinges on clear margins and the patient's overall health.
Radiation options
Stereotactic body radiation therapy (SBRT) delivers a high dose to a precise spot, sparing surrounding tissue. It works well for painful bone lesions or small lung nodules that are hard to resect.
Clinical trials why they matter
Because metastatic sarcoma is rare, many breakthroughs happen inside trial protocols. Participating can give access to novel agents like CDK4/6 inhibitors, oncolytic viruses, or even CAR-T cells designed for sarcoma antigens. A quick search on will reveal dozens of active studies.
Balancing benefits and risks
Every treatment carries a tradeoff. Chemotherapy can shrink tumors but may cause hair loss, fatigue, or heart strain. Targeted drugs often bring skin rashes or hypertension. Discussing your personal prioritiestime with family, quality of life, willingness to travel for carehelps the team craft a plan that feels right for you.
Can It Be Cured?
The current reality
For most patients with widespread disease, cure is not a realistic expectation. However, control is possiblemeaning you can keep the cancer at bay long enough to enjoy meaningful moments.
When longterm remission is possible
Rarely, patients with a single lung metastasis, good performance status, and complete surgical removal enjoy disease-free intervals that stretch beyond five years. These cases underscore why aggressive multimodal treatment (chemo + surgery + radiation) is still worth exploring when feasible.
Emerging research
Scientists are now testing engineered T-cells (CAR-T) that target sarcoma-specific proteins, and bispecific antibodies that bring immune cells directly to the tumor. While still experimental, early reports hint at deeper, more durable responses.
Living With Sarcoma
Palliative care integration
Palliative care isn't just for the end of life; it's a team that helps manage pain, shortness of breath, and emotional distress from day one. Studies show that patients who start palliative services early report better quality of life and sometimes even live longer.
Nutrition and gentle exercise
Maintaining muscle mass can improve tolerance to chemotherapy. Aim for protein-rich foodslean meats, beans, Greek yogurtand try short walks or light resistance bands as tolerated. The offers practical tips for cancer-related nutrition.
Financial and legal assistance
Medical bills, loss of income, and travel costs add up quickly. Nonprofits like the Sarcoma Foundation of America provide grants, and many hospitals have social workers who can help navigate insurance and disability paperwork.
Community support
Connecting with other families facing metastatic sarcoma can be a lifeline. Online forums, local support groups, and charity events let you share stories, ask practical questions, and feel less isolated.
Take Action Today
Ask your oncologist the right questions
Write down queries before appointments: What's my tumor's specific histology?, Are there clinical trials that match my profile?, What side-effects should I watch for with the proposed regimen? Feeling prepared makes the conversation smoother.
Bookmark reliable sources
Trusted sitesNCCN Guidelines, the National Cancer Institute, and major academic hospitalskeep their information up to date. Avoid anecdotal advice from unverified blogs.
Seek a second opinion
Because sarcoma treatment is highly specialized, getting a second opinion from a dedicated sarcoma center (often a major university hospital) can confirm the plan or reveal alternative approaches you hadn't considered.
Remember, you don't have to walk this path alone. Armed with the right knowledge, a supportive team, and a clear plan, you can make the most of each day and keep hope alive.
What's your biggest concern right now? Share your thoughts in the comments, or reach out if you need help finding resourcesyou're not alone.
FAQs
What are the most common signs that sarcoma has spread?
New persistent pain, unexplained weight loss, shortness of breath, a growing lump, or bone pain that occurs without injury can all indicate metastatic soft tissue sarcoma.
How do doctors confirm that the cancer has metastasized?
Diagnosis relies on imaging (CT of the chest, whole‑body PET‑CT, MRI for bone/soft‑tissue lesions) followed by a CT‑guided core needle biopsy to verify the tumor type and any molecular targets.
What systemic therapies are used for stage IV sarcoma?
The standard first‑line is an anthracycline‑based regimen such as doxorubicin ± ifosfamide. After progression, options include the VEGF inhibitor pazopanib, selected checkpoint inhibitors, or enrollment in clinical trials.
Which factors most affect life expectancy in metastatic sarcoma?
Key factors are the number and location of metastases, histologic grade, patient performance status, and how well the tumor responds to the initial chemotherapy.
Can participating in clinical trials improve outcomes?
Yes—trials provide access to novel agents (e.g., CDK4/6 inhibitors, CAR‑T cells, bispecific antibodies) that are not yet widely available and may offer longer disease control for eligible patients.