Got a scan that shows something odd in your lungs? Youre probably wondering what the next step is, and yes, that often means a lung biopsy. In the next few minutes, Ill walk you through the main lung biopsy types, the goodandbad bits of each, and what you can realistically expect before, during, and after the procedure. Think of this as a friendly chat over coffeeno jargon, just straighttothepoint info.
Overview of Options
First things first: there isnt just one lung biopsy. Doctors have a toolbox of techniques, each suited to a different situation. Below is a quick snapshot of the most common methods.
| Method | How Its Done | Typical Setting | Main Use Cases |
|---|---|---|---|
| Percutaneous (Transthoracic) Needle Biopsy | Thin needle pushed through the chest wall under CT or ultrasound guidance | Radiology suite | Peripheral nodules that cant be reached by a bronchoscope |
| Transbronchial Lung Biopsy (TBLB) | Bronchoscope slips through the airways; tiny forceps snip a sample | Endoscopy unit | Central lesions and diffuse lung disease |
| VideoAssisted Thoracoscopic Surgery (VATS) / Thoracoscopic Biopsy | Small incisions, camera, and instruments remove tissue | Operating room (minimally invasive) | Larger samples, suspicious lesions, staging of cancer |
| Open Lung Biopsy | Full chest opening; surgeon removes a piece of lung | Operating room (traditional surgery) | When other methods arent conclusive or need a big sample |
| FineNeedle Aspiration (FNA) / Core Needle | Very thin needlesometimes needleonlydraws cells | Radiology suite | Quick diagnosis of lowrisk lesions |
Sources like and the StatPearls article on lung biopsy back up these descriptions.
Common Questions Answered
What is a lung biopsy and why is it performed?
A lung biopsy is simply a way to grab a tiny piece of lung tissue so pathologists can look at it under a microscope. The goal? Confirm whether a spot is cancer, infection, inflammation, or something else. Without that microscopic proof, doctors are often left guessing, which can delay the right treatment.
How many lung biopsy types exist?
In everyday practice youll hear about five: percutaneous needle, transbronchial, VATS (or thoracoscopic), open, and fineneedle aspiration. Each has its own pros and cons, which well break down shortly.
Which lung biopsy type is the most common?
That title belongs to the percutaneous transthoracic needle biopsy. Its quick, done outpatient, and works for most peripheral nodulesexactly why radiologists love it.
Can a lung biopsy cause cancer to spread?
Its a fair fear. The technical term is tumor seeding, and studies show its rareroughly 0.5% to 2% of cases, depending on the needle size and tumor type. Doctors take precautions like using the smallest effective needle and planning the track to avoid breaching the pleura whenever possible.
Is a lung biopsy a serious procedure?
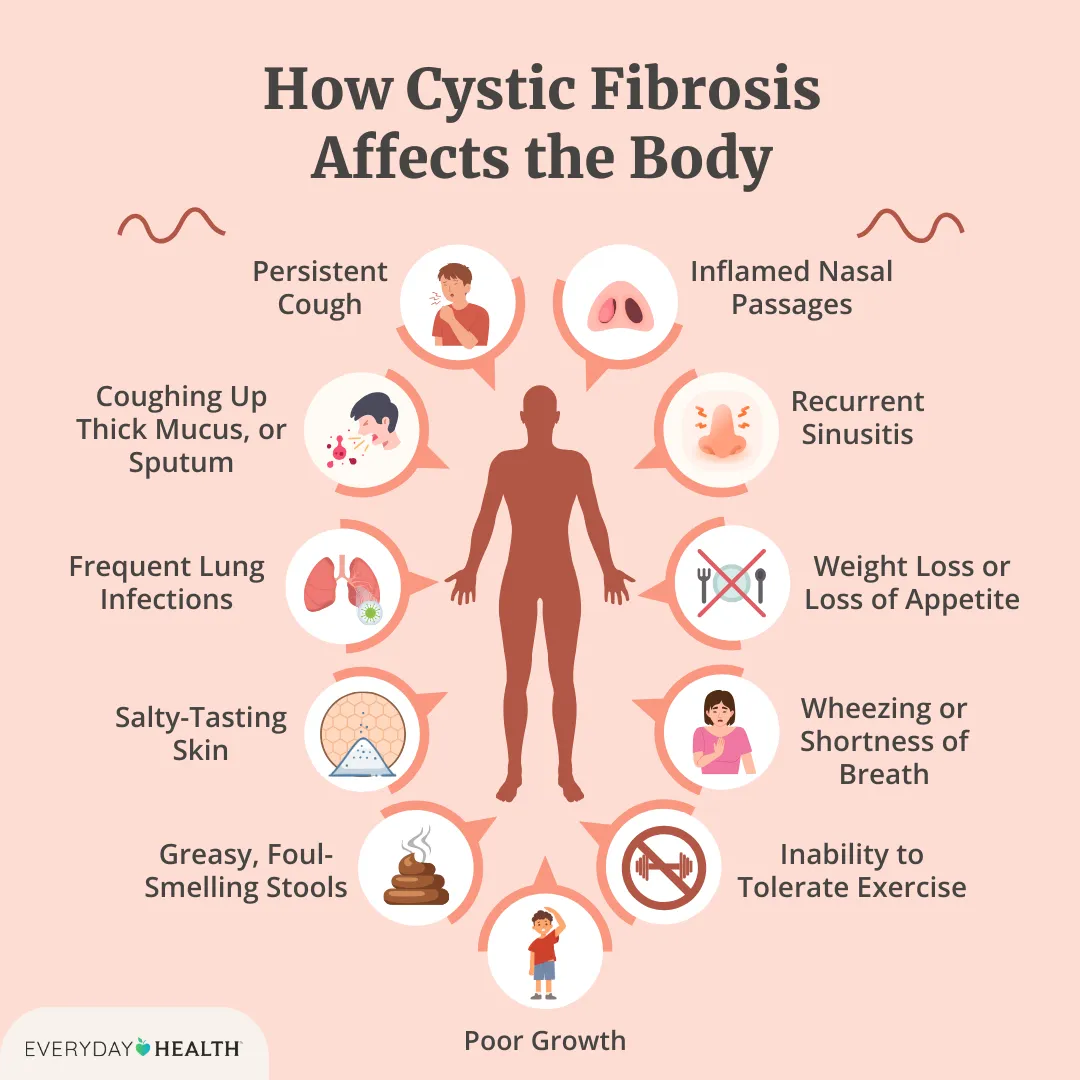
Seriousness is relative. A needle biopsy is minimally invasive, often done with just local anesthesia, while an open biopsy is a major operation requiring general anesthesia and a hospital stay. The key is matching the method to your health status and the diagnostic need. For those with underlying lung conditions, such as cystic fibrosis, the situation may be more complex, and discussions about cystic fibrosis safety should be had with your care team to assess procedural risk and recovery.
What is the most common complication of a lung biopsy?
That would be a pneumothoraxa little air leak that makes the lung collapse a bit. For needle biopsies, the rate hovers around 15%25%, but most are small and resolve with a brief observation or a quick needle tap to release the air.
How painful is a lung biopsy?
Most patients report mild to moderate discomfortthink of a quick pinch followed by a short ache that fades within a day. The pain score usually lands between 2 and 4 on a 010 scale, especially when you get a local anesthetic or light sedation.
What are the risks for elderly patients?
Age alone isnt a dealbreaker, but older folks often have weaker lungs, heart issues, or bloodthinner meds that raise the chance of bleeding or pneumothorax. In such cases, physicians may favor a bronchoscopy or a VATS approach because they can control the environment better.
How long is lung biopsy recovery time?
Recovery varies by method:
- Needle biopsy: Most people go home the same day; full activity can resume within 24hours.
- Transbronchial: Observation for 612hours; normal routine in 12days.
- VATS: Hospital stay 12days; mild soreness for a week.
- Open biopsy: 35days in the hospital, with 12weeks of limited activity.
When will I get lung biopsy results?
For cytology (cell studies) you might hear back in 23days. A full pathology report, especially when immunohistochemistry is needed, often takes 510days. Your doctor will let you know the exact timeline.
Benefits vs Risks
QuickReference Table
| Type | Benefits | Risks / Complications | Pain (010) | Recovery |
|---|---|---|---|---|
| Percutaneous Needle | Outpatient, minimal incision | Pneumothorax, bleeding, rare tumor seeding | 23 | Sameday to 24h |
| Transbronchial (TBLB) | Access to central lesions, no chest wall puncture | Bleeding, infection, limited sample size | 24 | 2448h |
| VATS / Thoracoscopic | Larger tissue, high diagnostic yield | General anesthesia, infection, longer stay | 46 | 35days |
| Open Biopsy | Definitive diagnosis when others fail | Major surgery risks, longer hospitalization | 68 | 714days |
| FineNeedle Aspiration | Fast, lowrisk | Potentially inconclusive, may need repeat | 12 | Sameday |
DecisionMaking Flowchart (Simplified)
Picture a tiny decision tree in your mind:
- Location of the lesion? Peripheral think needle or FNA. Central bronchoscopy or VATS.
- Hows your overall health? High surgical risk stick with needle or bronchoscopy.
- Need a big tissue piece? Yes VATS or open; No needle/FNA.
- How fast do you need an answer? Immediate onsite cytology with needle biopsy.
For patients with respiratory conditions involving mucus clearance problems, such as those needing cystic fibrosis airway clearance, these factors may require specialized care coordination before and after lung biopsy procedures.
RealWorld Snapshots (Experience)
Case 1 68yearold former smoker: A small 1cm nodule showed up on his CT. The team chose a percutaneous needle biopsy. He felt a brief pinch, lay in the recovery chair for an hour, and was home by lunchtime. Pathology revealed earlystage adenocarcinoma, and he started curative surgery within weeks.
Case 2 74yearold with COPD: Because her lungs were already floppy, the pulmonologist opted for a thoracoscopic VATS biopsy. She liked the idea of a slightly bigger incision if it meant a lower chance of a pneumothorax. She spent two nights in the hospital, reported mild soreness, and was back to light walking in four days.
Preparing for the Procedure
Preprocedure checklist
- Bring recent imaging (CT, PET) and a list of medications.
- Stop blood thinners (aspirin, warfarin, clopidogrel) as directedusually 57days earlier.
- Fast if youll receive sedation (usually nothing solid for 6hours).
- Ask your doctor about any allergies to contrast dye or anesthesia.
Dayofprocedure timeline
- Checkin and consent signing (yes, those forms are important!).
- IV line placement, vital sign monitoring.
- Local anesthetic or light sedation administered.
- Biopsy performedmost take 1030minutes.
- Observation period: a quick chest Xray for needle biopsies to rule out pneumothorax.
- Discharge instructions (when to call the doctor, activity limits, breathing exercises).
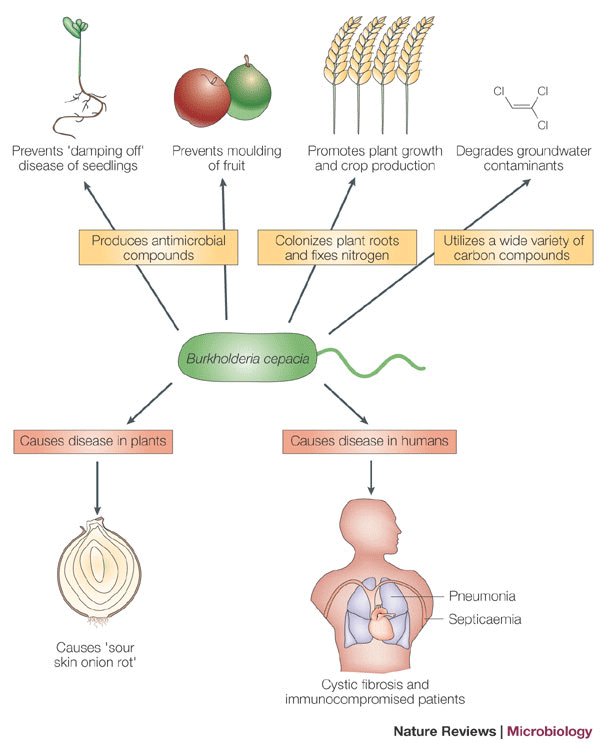
Some individuals with underlying lung diseases must pay special attention to preventing infectious complications and cross-infection. For example, those with CF are often advised about cf social distance, which can impact both their hospital stay and post-procedure precautions.
Postprocedure care tips
- Breathing exercises: Gentle diaphragmatic breathing helps reinflate the lung if a tiny air leak occurs.
- Activity: Light walking is encouraged; avoid heavy lifting or vigorous exercise for at least 24hours after a needle biopsy.
- Warning signs: Sudden shortness of breath, sharp chest pain, or coughing up bloodcall your doctor or go to the ER.
- Followup imaging: A chest Xray is often done the next morning to ensure the lung is fully expanded.
Conclusion
Choosing the right lung biopsy type isnt about picking the most hightech gadget; its about balancing what the doctor needs to see with whats safest for you. Whether you end up with a quick needle stick, a bronchoscope sailing through your airways, or a small thoracoscopic operation, the goal is the same: get a clear diagnosis so you can move forward with confidence.
Now that youve got the layoftheland, you can have a more informed conversation with your pulmonologist or thoracic surgeon. Ask about the specific risks, recovery expectations, and why a particular method fits your situation. Your health journey is personal, and a little knowledge goes a long way in making it smoother.
Whats your experience with a lung biopsy, or what worries you most? Share your thoughts in the commentstalking it out helps everyone feel less alone. And if you have any lingering questions, dont hesitate to ask your care team; theyre there to guide you every step of the way.
FAQs
What are the main types of lung biopsy?
The common methods are percutaneous (transthoracic) needle biopsy, transbronchial lung biopsy (via bronchoscope), video‑assisted thoracoscopic surgery (VATS), open surgical biopsy, and fine‑needle aspiration (FNA) or core needle biopsy.
How long does recovery take after a percutaneous lung biopsy?
Most patients go home the same day and can resume normal activities within 24 hours, although a brief observation period (often 1–2 hours) is standard to ensure no pneumothorax develops.
Is a lung biopsy painful?
With local anesthesia or light sedation, pain is usually mild to moderate—similar to a pinprick followed by a short ache that generally fades within a day (pain score 2–4/10).
Can a lung biopsy cause a pneumothorax?
Yes, air leakage is the most common complication, occurring in about 15‑25 % of needle biopsies. Most cases are small and resolve with a brief needle “tap” or observation; larger leaks may need a chest tube.
When will I receive the biopsy results?
Cytology results may be available in 2‑3 days, while a full pathology report with immunohistochemistry typically takes 5‑10 days.