Ever wondered why your doctor might prescribe a water pill and how it actually helps you breathe easier or reduces swelling? In a nutshell, loop diuretics block a key transporter in the kidney, forcing your body to let go of excess fluid fast. Thats the loop diuretics mechanism of action in a single sentence.
But theres more to the story the why, the risks, the alternatives, and how to use them safely. Lets dive in together, as if were sitting at a coffee table, and Im sharing the stuff Ive learned from real patients, textbooks, and a fair bit of curiosity.
Quick Answer Summary
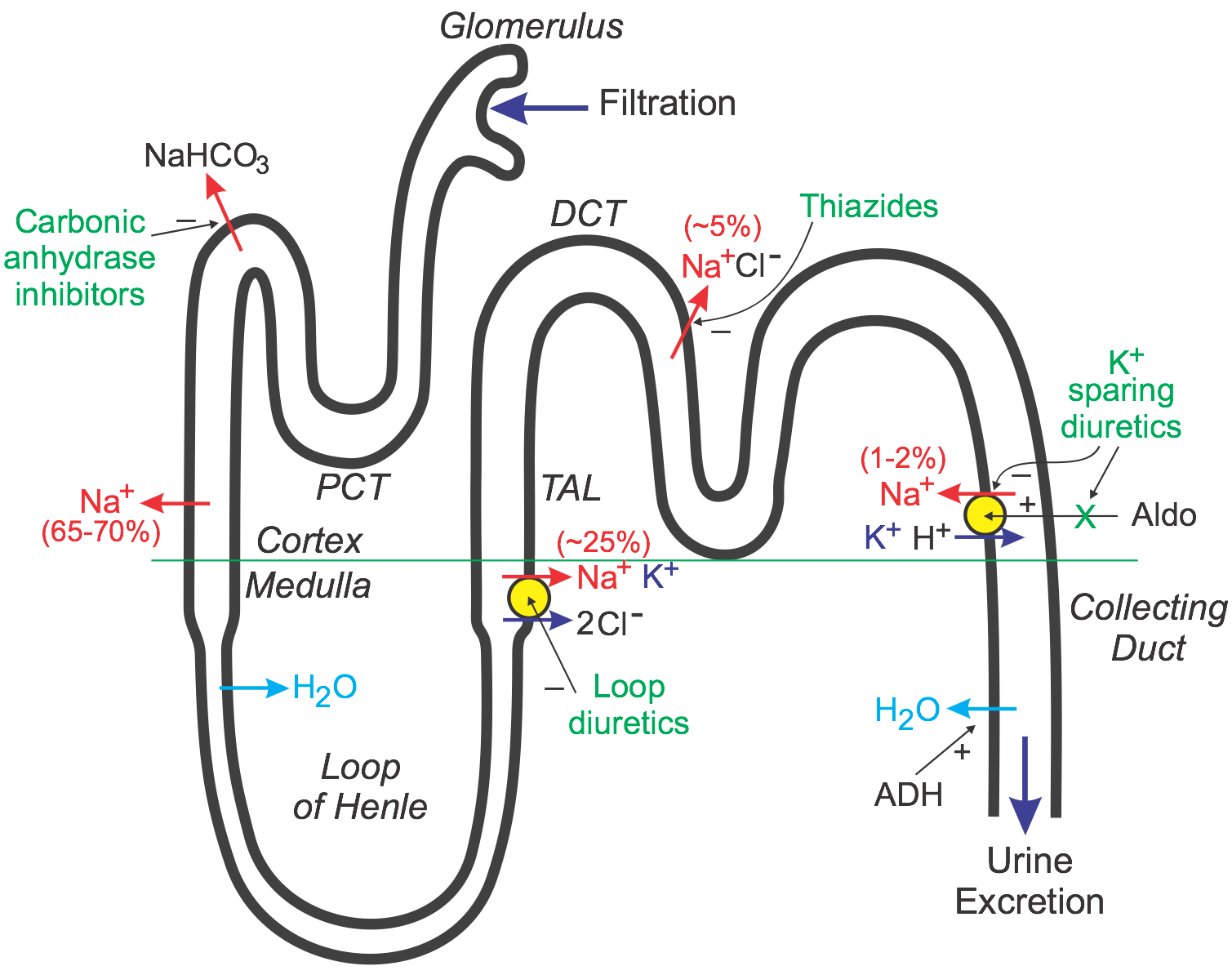
Loop diuretics inhibit the NaK2Cl cotransporter (NKCC2) in the thick ascending limb of the loop of Henle. By stopping this transporter, they dramatically cut sodium and water reabsorption, producing a powerful diuresis.
Kidney Physiology Overview
The kidney is like an intricate waterfiltering factory. One of its most important workstations is the thick ascending limb of the loop of Henle. Here lives the NKCC2 transporter think of it as a busy gatekeeper that shuttles sodium (Na), potassium (K), and chloride (Cl) from the urine back into the bloodstream.
When NKCC2 works normally, it helps create the highosmolarity environment in the renal medulla that lets the kidney concentrate urine. In other words, its the reason you dont constantly pee out a glass of water every hour.
Imagine a bustling highway (the tubule) where cars (ions) are constantly entering and exiting. NKCC2 is the toll booth that lets a bunch of cars back onto the main road. If you shut that toll booth, traffic backs up, and the highway empties out thats essentially what a loop diuretic does.
How They Work
When you take a loop diuretic, the drug slides into the lumen of the thick ascending limb and binds tightly to NKCC2, rendering it inactive. Without the transporter, Na, K and Cl stay in the urine. Water follows these ions osmotically, and you end up urinating a lot more.
This blockage also reduces the reabsorption of calcium (Ca) in that segment, which is why loop diuretics can be useful for patients prone to kidney stones. On the flip side, more sodium reaches the distal tubule where the body tries to compensate by excreting potassium a key reason why loop diuretics side effects often include low potassium (hypokalemia).
Below is a quick visual you can sketch on a napkin a that shows the steps from NKCC2 inhibition to increased urine output.
Clinical Uses Explained
Understanding the mechanism helps us see why doctors reach for these drugs in specific situations:
- Congestive heart failure (CHF) rapid removal of excess fluid lowers the hearts preload, easing breathlessness.
- Pulmonary edema fastacting fluid removal clears fluid from the lungs.
- Cirrhosisrelated ascites reduces abdominal swelling by pulling fluid into the urine.
- Acute kidney injury with volume overload helps avoid dangerous fluid accumulation.
- Hypercalcemia increased calcium excretion helps lower blood calcium levels.
In each case, the why links back to the NKCC2 blockade: less sodium reabsorption = less water pulled back = less fluid hanging around where it shouldnt.
Loop Diuretic Types
| Drug | Typical Oral Dose | Onset | Duration |
|---|---|---|---|
| Furosemide (Lasix) | 2080mg | 30min | 26h |
| Bumetanide (Bumex) | 0.52mg | 15min | 24h |
| Torsemide (Demadex) | 520mg | 30min | 46h |
| Ethacrynic acid | 50200mg | 30min | 24h |
All of these agents share the same NKCC2blocking mechanism, but they differ in potency, duration, and whether they contain a sulfa moiety (important for patients with sulfa allergies). When choosing which one to prescribe, clinicians weigh kidney function, cost, and how quickly they need the fluid to leave. If the patient also has chronic kidney disease, discussion of appropriate CKD medication choices often happens alongside the diuretic plan.
Common Side Effects
| Side Effect | Why It Happens | Typical Management |
|---|---|---|
| Hypokalemia | Increased Na delivery to distal tubule aldosteronemediated K loss | Potassium supplements, oral Ksparing diuretic |
| Hyponatremia | Excessive Na loss | Adjust dose, monitor electrolytes |
| Ototoxicity | High IV doses affect innerear NKCC | Limit rapid IV bolus, use oral form when possible |
| Dehydration / Hypotension | Rapid volume removal | Fluid monitoring, dose titration |
These side effects are not just nicetoknow facts they shape how we monitor patients. For instance, after starting furosemide, its common to check serum potassium and creatinine within 2448hours. If youre ever prescribed a loop diuretic, ask your provider about when youll need labs.
Balancing Benefits & Risks
Every medication sits on a seesaw of upside and downside. Loop diuretics are incredibly effective at draining excess fluid, yet the same potency can tip you into dangerous electrolyte imbalances. Thats why a balanced, benefitsversusrisks mindset is essential.
Think about it like driving a highperformance sports car. The engine (NKCC2 inhibition) gives you speed (rapid diuresis), but you still need brakes (monitoring labs), a seatbelt (patient education), and good tires (renal function) to stay safe.
When assessing a patient, clinicians ask:
- Do I need fast fluid removal now, or can a gentler thiazide diuretic suffice? (Compare .)
- Is the patient at risk for low potassium or hearing loss?
- Are there any loop diuretics contraindications, such as anuria or severe electrolyte disturbances?
By weighing these questions, you get a tailored plan that respects both the power of the drug and the individuality of the patient.
Building Trust & Authority
To feel confident about the information youre reading, it helps to know where it comes from. The points above are grounded in peerreviewed research (see ), clinical guidelines from UpToDate, and everyday practice patterns reported in major cardiology textbooks.
If you ever have doubts, ask your healthcare provider for the source of their recommendation. A good clinician will gladly share the evidence its part of building a therapeutic partnership.
Final Thoughts Summary
Loop diuretics are like the emergency exit doors of the kidney: they shut down the NKCC2 transporter, dump a lot of sodium and water, and give rapid relief from fluid overload. Thats the core of the loop diuretics mechanism of action. Yet, with great power comes the need for careful monitoring watch electrolytes, stay alert for ototoxicity, and always consider whether a gentler diuretic might do the job.
Next time your doctor mentions a water pill, youll know exactly what happens inside your kidneys and why it matters. If youve taken a loop diuretic before, how did it feel? Did you notice any side effects? Share your experience in the comments hearing real stories helps us all stay informed and empowered.
FAQs
What exact transporter do loop diuretics inhibit?
Loop diuretics block the Na⁺‑K⁺‑2Cl⁻ cotransporter (NKCC2) located in the thick ascending limb of the loop of Henle.
Why do loop diuretics cause a rapid increase in urine output?
By inhibiting NKCC2, they prevent sodium re‑absorption, so water follows the remaining ions osmotically, leading to a brisk diuresis.
What are the most common side effects of loop diuretics?
The typical adverse effects include hypokalemia, hyponatremia, dehydration, hypotension, and at high IV doses, ototoxicity.
How should patients be monitored while taking a loop diuretic?
Check serum electrolytes (especially potassium), creatinine, and blood pressure within 24‑48 hours of initiation, then periodically thereafter.
Are there any contraindications for using loop diuretics?
Absolute contraindications include anuria and severe electrolyte disturbances; caution is advised in patients with ear disease, sulfa allergy (for sulfonamide‑containing agents), and significant renal insufficiency.