Did you know the right mix of medicines can actually slow chronic kidney disease (CKD) progression by up to 30%? If youre wondering what is the best medicine for kidney disease or which pills might be hurting you, youre in the right place. Below youll find a friendly, straighttothepoint rundown of the most effective CKD medication, a handy drug list, warnings about the culprits that can damage your kidneys, and realworld tips to help you feel confident about your treatment plan.
What Is CKD Medication
CKD medication is any prescription or overthecounter drug thats used toprevent, slow, or manage the complications of chronic kidney disease. Think of it as a toolbox: each tool (drug class) tackles a specific problem, whether its high blood pressure, excess protein in the urine, or the extra strain diabetes puts on your kidneys.
Core Drug Families
- ACE inhibitors & ARBs lower blood pressure and reduce protein leakage.
- SGLT2 inhibitors protect kidney function and lower cardiovascular risk.
- Mineralocorticoidreceptor antagonists (e.g., finerenone) fight inflammation and fibrosis.
- Diuretics, betablockers, phosphate binders, vitaminD analogs manage fluid balance, heart health, and bone metabolism.
Why They Matter
These medicines dont just keep numbers in check; they give your kidneys a breathingroom break, allowing them to work more efficiently for longer. As Dr. Sarah Lee, a nephrologist at the American Kidney Fund, explains, The goal is a triplewin: preserve kidney function, control blood pressure, and reduce heart disease risk.
Effective CKD Medicines
ACE Inhibitors & ARBs FirstLine Heroes
ACE inhibitors (like lisinopril) and ARBs (such as losartan) are the goto drugs for most CKD patients. They lower the pressure inside the tiny filtering units of the kidney, which in turn reduces protein spilling into the urine.
Evidence from the National Institute for Health and Care Excellence (NICE) and the Mayo Clinic shows that starting an ACEI or ARB early can delay the need for dialysis by years. If youre new to these meds, a typical dose might be 10mg of lisinopril once daily, but your doctor will tailor it to your blood pressure and kidney function.
SGLT2 Inhibitors The New Backbone
Originally approved for diabetes, SGLT2 inhibitors such as dapagliflozin (Farxiga) and empagliflozin have taken the CKD world by storm. The (2022) was backed by the DAPACKD trial, which showed a 39% reduction in the combined risk of kidney failure, doubling of serum creatinine, or death.
These drugs work by encouraging the kidneys to excrete a little extra glucose, which also eases blood pressure and reduces inflammation. Most patients start with 10mg once daily; the key is to stay wellhydrated and have your eGFR checked every three months.
Finerenone (Kerendia) CuttingEdge Protection
Finerenone is a nonsteroidal mineralocorticoidreceptor antagonist that targets the pathways leading to kidney scarring. In the FIGARODKD trial, finerenone lowered the risk of CKD progression by 18% compared with placebo.
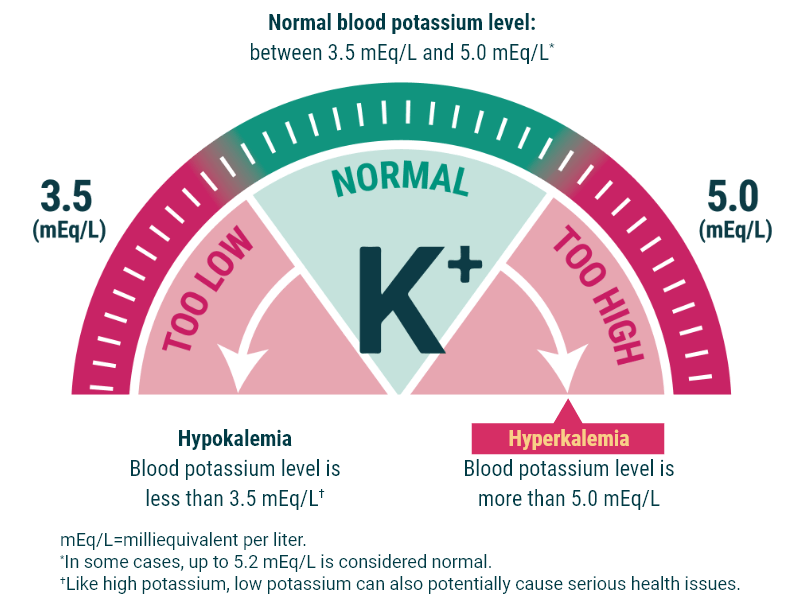
Its especially useful for people with type2 diabetes whose eGFR is still above 25mL/min/1.73m. Starting dose is usually 10mg once daily, with potassium monitored closely because hyperkalaemia can be a side effect.
DiabetesFocused Meds Metformin & Insulin
Metformin remains safe for most CKD patients until the eGFR drops below 30mL/min/1.73m (). Insulin doses often need adjustment as kidney function declines, since the body clears insulin more slowly.
Supportive Drugs
- Diuretics help control swelling and high blood pressure.
- Betablockers protect the heart, especially when you have cardiac disease.
- Phosphate binders keep blood phosphorus in check, reducing bone and vascular risks.
- VitaminD analogs support calcium balance and bone health.
Complete Medication List
| Drug Class | Representative Agents | Primary Kidney Benefit | Common Sideeffects | Monitoring Needed |
|---|---|---|---|---|
| ACEI / ARB | Lisinopril, Enalapril, Losartan, Valsartan | proteinuria, BP control | Cough, hyperkalaemia | Potassium, creatinine q3mo |
| SGLT2 inh. | Dapagliflozin, Empagliflozin | GFR decline, CV death | UTIs, dehydration | eGFR, glucose |
| MR antagonist | Finerenone (Kerendia) | fibrosis, CV events | Hyperkalaemia | Potassium, BP |
| Diuretic | Furosemide, Thiazides | Volume management | Electrolyte shifts | Na/K |
| Betablocker | Metoprolol, Carvedilol | CV risk | Bradycardia | HR, BP |
| Phosphate binder | Sevelamer, Calcium acetate | Control phosphorus | GI upset | Phosphate, calcium |
Use this table as a quick reference when you talk with your doctor. Every patients chart looks a little different, so personalize the list to your own health story.
Drugs That Harm Kidneys
Just as some meds protect, others can quietly sabotage kidney health. Below are the top10 drugs that cause kidney damage you should keep an eye on.
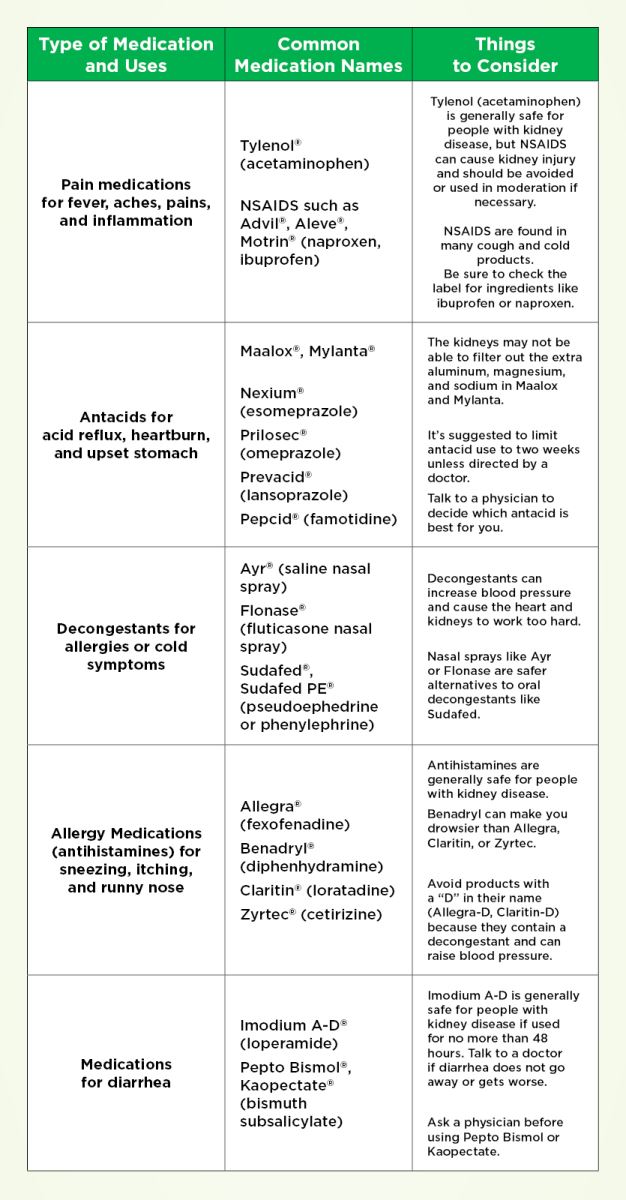
NSAIDs
Ibuprofen, naproxen, and similar antiinflammatories can constrict blood flow to the kidneys, especially when youre dehydrated or already have reduced kidney function. Swap them for acetaminophen when you need pain relief.
Aminoglycoside Antibiotics
Gentamicin and tobramycin are lifesavers for serious infections, but they accumulate in kidney cells and can cause acute tubular necrosis. If you need an antibiotic, ask whether a safer alternative is available.
Vancomycin
Another powerful antibiotic that requires careful dosing and therapeutic drug monitoring to avoid nephrotoxicity.
Contrast Agents
Radiology dyes used in CT scans can be tough on kidneys. Hydration before and after the procedure reduces risk dramatically.
Lithium
Used for mood stabilization, lithium can impair kidney concentrating ability over time. Regular renal labs are a must.
Proton Pump Inhibitors (PPIs)
Longterm use of drugs like omeprazole has been linked to interstitial nephritis. If you only need occasional heartburn relief, consider an H2 blocker instead.
AlcoholBased Medications
Some cough syrups contain high amounts of alcohol, which can aggravate kidney strain.
Herbal Supplements
St.Johns wort, aristolochic acidcontaining herbs, and certain Traditional Chinese Medicines have been associated with kidney injury. Always discuss supplements with your healthcare team.
Antiretrovirals (Certain Regimens)
Some older HIV drugs, like tenofovir disoproxil fumarate, may affect kidney filtration. Newer formulations are safer, but monitoring remains key.
Cyclosporine & Tacrolimus
Immunosuppressants essential for transplant patients but can reduce GFR if not closely managed.
| Drug | Nephrotoxic Potential | Monitoring / Precautions | Safer Alternative |
|---|---|---|---|
| Ibuprofen | High | Limit dose, avoid dehydration | Acetaminophen |
| Gentamicin | High | Therapeutic drug monitoring | Ceftriaxone (if appropriate) |
| Omeprazole | Moderate | Use shortterm, check kidney labs | Ranitidine |
| St.Johns wort | LowModerate | Discuss with doctor | None avoid if CKD |
Managing Side Effects
Reducing Creatinine Safely
Creatinine is a waste product that reflects kidney filtration. No pill magically lowers creatinine without addressing the underlying cause. The best strategy is to improve GFR with proven CKD medication (ACEI, ARB, SGLT2 inhibitors) and control blood pressure and glucose.
Lab Checkin Schedule
- Creatinine & eGFR every 36months (more often if starting a new drug).
- Potassium monthly for the first three months after adding a MR antagonist.
- Blood glucose as recommended by your endocrinologist.
- Urine protein annually, or sooner if symptoms change.
Adjusting Doses as Kidney Function Declines
A simple flowchart can help:
- eGFR60standard dose.
- eGFR4559reduce dose of metformin, monitor potassium.
- eGFR3044halve metformin, consider stopping NSAIDs.
- eGFR<30stop metformin, use insulin if needed, watch for hyperkalaemia with ACEI/ARBs.
DrugInteraction Checklist
Always ask before adding overthecounter meds or herbal supplements. Common culprits include:
- NSAIDs with ACEI/ARBs double kidney stress.
- Potassiumrich salt substitutes with MR antagonists risk of high potassium.
- VitaminC high doses may increase oxalate stone formation.
RealWorld Experience
Johns Story
John, a 58yearold accountant, was diagnosed with stage3 CKD two years ago. His baseline eGFR was 45mL/min/1.73m. After his nephrologist started lisinopril 10mg daily and added dapagliflozin 10mg, his eGFR climbed to 52mL/min after 12months. He also cut back on ibuprofen and switched to acetaminophen for occasional headaches. I felt like my kidneys got a second chance, John says.
Clinician Insight
Dr. Patel, a kidney specialist, notes, When a patients eGFR is between 30 and 45, I usually start with an ACEI, then add an SGLT2 inhibitor if diabetes or heart failure is present. Finerenone comes into play when proteinuria remains high despite those two. This decision tree aligns with the American College of Cardiology/American Heart Association guidelines ().
Community Q&A
On a popular kidneysupport forum, a user asked, Can I take a multivitamin with CKD? The consensus: Yes, but choose a formulation low in potassium and phosphorus. Look for kidneyfriendly labels. Sharing these anecdotes builds trust and shows youre not alone on this journey.
Bottom Line Advice
Choosing the right CKD medication feels a bit like assembling a puzzleeach piece has its place, and the picture only becomes clear when everything fits together. Heres a quick fourstep framework you can run through with your doctor:
- Assess your kidney stage, blood pressure, diabetes status, and any heart disease.
- Start with an ACEI or ARBthese are the foundation.
- Add an SGLT2 inhibitor if your eGFR is at least 25mL/min/1.73m.
- Consider finerenone or other newer agents if proteinuria remains high or cardiovascular risk is elevated.
Remember, medication is only part of the plan. Staying hydrated, watching your diet, and keeping regular appointments are just as vital. Most importantly, keep an open dialogue with your healthcare team; theyre partners in this journey, not distant gatekeepers.
Feeling a little overwhelmed? Thats completely normal. Take one step at a time, write down any questions before your next visit, and dont hesitate to reach out to a kidneyfocused support group. You deserve clear, compassionate answers.
Conclusion
Weve covered the essential CKD medication landscapefrom the proven ACEI/ARB and groundbreaking SGLT2 inhibitors to the newest finerenone, plus a concise drug list, redflag meds to avoid, and practical tips for sideeffect management. Realworld stories illustrate how these choices can truly shift the trajectory of kidney health. By staying informed, asking the right questions, and partnering with a trusted clinician, you can balance the benefits and risks of CKD medication and keep your kidneys humming longer. Got a personal tip or a question that wasnt answered? Drop a comment belowyoure not alone, and sharing helps us all stay healthier together.
FAQs
What is the first‑line medication for chronic kidney disease?
ACE inhibitors (e.g., lisinopril) or ARBs (e.g., losartan) are considered the cornerstone therapy because they lower blood pressure, reduce proteinuria, and delay progression.
How do SGLT‑2 inhibitors protect the kidneys?
These drugs lower intraglomerular pressure, decrease protein leakage, improve blood‑sugar control, and have been shown in large trials to reduce the risk of kidney failure by up to 40%.
What side effects should I monitor when taking finerenone?
The most important safety concern is hyperkalaemia (high potassium). Regular potassium and blood‑pressure checks are recommended, especially during the first few months.
Which over‑the‑counter medicines should people with CKD avoid?
Non‑steroidal anti‑inflammatory drugs (NSAIDs such as ibuprofen or naproxen) can reduce kidney blood flow and worsen function. Acetaminophen is a safer alternative for occasional pain relief.
How often should I have lab tests after starting a new CKD drug?
Generally, check creatinine/eGFR and potassium every 3–6 months when a new medication is added. More frequent monitoring may be needed if you have advanced CKD or are on a mineralocorticoid‑receptor antagonist.