Answer 1: Yes a noticeable portion of people with cyclothymia may later meet the clinical criteria for BipolarI or II, but many stay stable with the right support.
Answer 2: Knowing why this can happen, spotting early warnings, and taking practical steps now can help you keep the mood rollercoaster under control.
Cyclothymia vs Bipolar
What exactly is cyclothymia?
Think of cyclothymia as a milder, longerlasting version of bipolar disorder. Instead of fullblown manic highs or deep depressive lows, you experience milder highish periods (often called hypomaniclike) and lowish periods that last for at least two years in adults. The swings are usually not severe enough to cripple daily life, but they can feel like an endless tugofwar.
How does bipolar differ?
Bipolar disorder splits into two main types:
- BipolarI: At least one full manic episode (extreme energy, risky behavior, little need for sleep) often followed by depressive episodes.
- BipolarII: At least one hypomanic episode plus at least one major depressive episode, but never a full mania.
Where does cyclothymia sit on the spectrum?
| Condition | Typical Episode Length | Severity | Impact on Function |
|---|---|---|---|
| Cyclothymia | Daysweeks | Mildmoderate | Usually manageable |
| BipolarII | Weeksmonths | Moderatesevere | Often disrupts work/relationships |
| BipolarI | Weeksmonths (mania) | Severe | Can be disabling without treatment |
In short, cyclothymia lives in the grey zone of the mooddisorder spectrum. Its not a guarantee youll slide into bipolar, but the transition is possible.
Conversion Rates Explained
What does research say?
Longterm studies suggest anywhere from 10% to 50% of people diagnosed with cyclothymia eventually meet criteria for BipolarI or II. A large communitybased followup published in the found a 27% conversion after ten years.
Why isnt there a single number?
Most of the data come from smallscale or retrospective studies, and diagnostic thresholds have shifted over the decades. Plus, many people never seek a formal diagnosis, so the realworld conversion may be higheror lowerthan what the papers show.
What does this mean for you?
Even if statistics sound daunting, remember theyre averages. Your personal risk hinges on genetics, lifestyle, and how proactively you manage symptoms.
Warning Signs to Watch
Highs getting higher?
If your up periods start lasting longer than a few days, or you notice:
- Sleeping less than four hours and still feeling wired
- Spending sprees, impulsive decisions, or risky sexual behavior
- Feeling invincible or overly grandiose
these could be the first hints that hypomania is edging toward true mania.
Low moments deepening?
When depressive phases become more than meh and you experience:
- Persistent sadness or irritability lasting weeks
- Thoughts of hopelessness or, in severe cases, suicidal ideation
- Significant drop in work or school performance
its a red flag that the mood swing pattern may be evolving.
New stressors or triggers?
Acute life eventslike a breakup, a new job, or a traumatic incidentcan act as catalysts. Even chronic stress, such as ongoing financial worries, can push the system over the edge.
Family history matters
Having a firstdegree relative with bipolar disorder roughly doubles your own risk. If mentalhealth issues run in your family, keep a closer eye on mood changes.
Quick selfmonitoring checklist
- Are my high periods longer or more intense than before?
- Do I need less sleep and still feel energetic?
- Has my low mood become more disabling?
- Are new stressors appearing in my life?
- Do I have a family history of bipolar?
Tick off the items each week. If a handful start turning green, consider reaching out to a clinician.
Triggers & Risk Factors
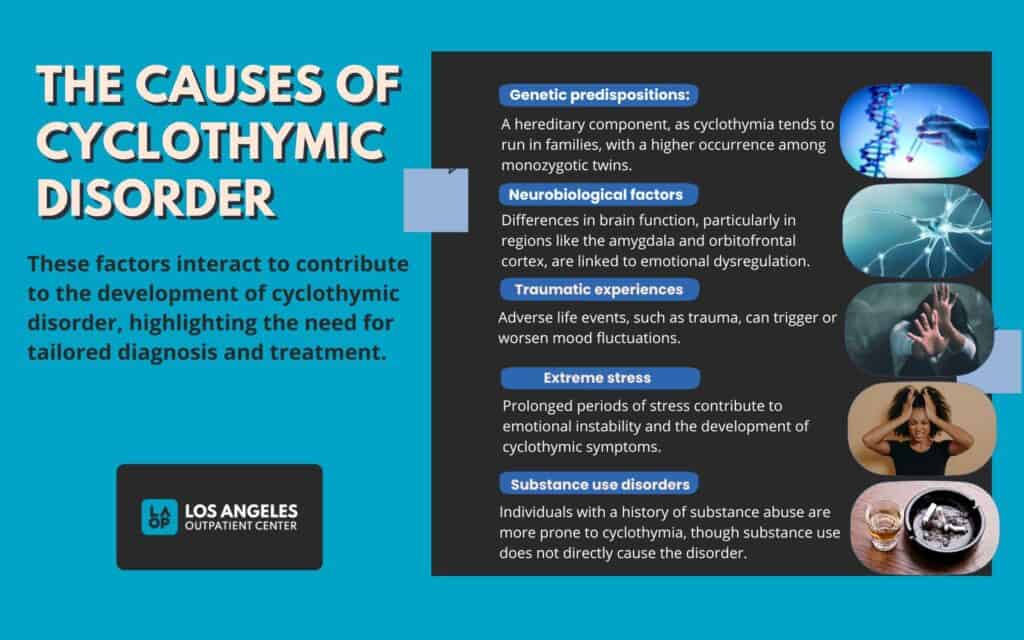
Biological underpinnings
Genetics play a major rolestudies show a 6080% heritability for bipolar spectrum disorders. Neurochemical imbalances, especially in dopamine and serotonin pathways, may also predispose certain individuals.
Environmental stressors
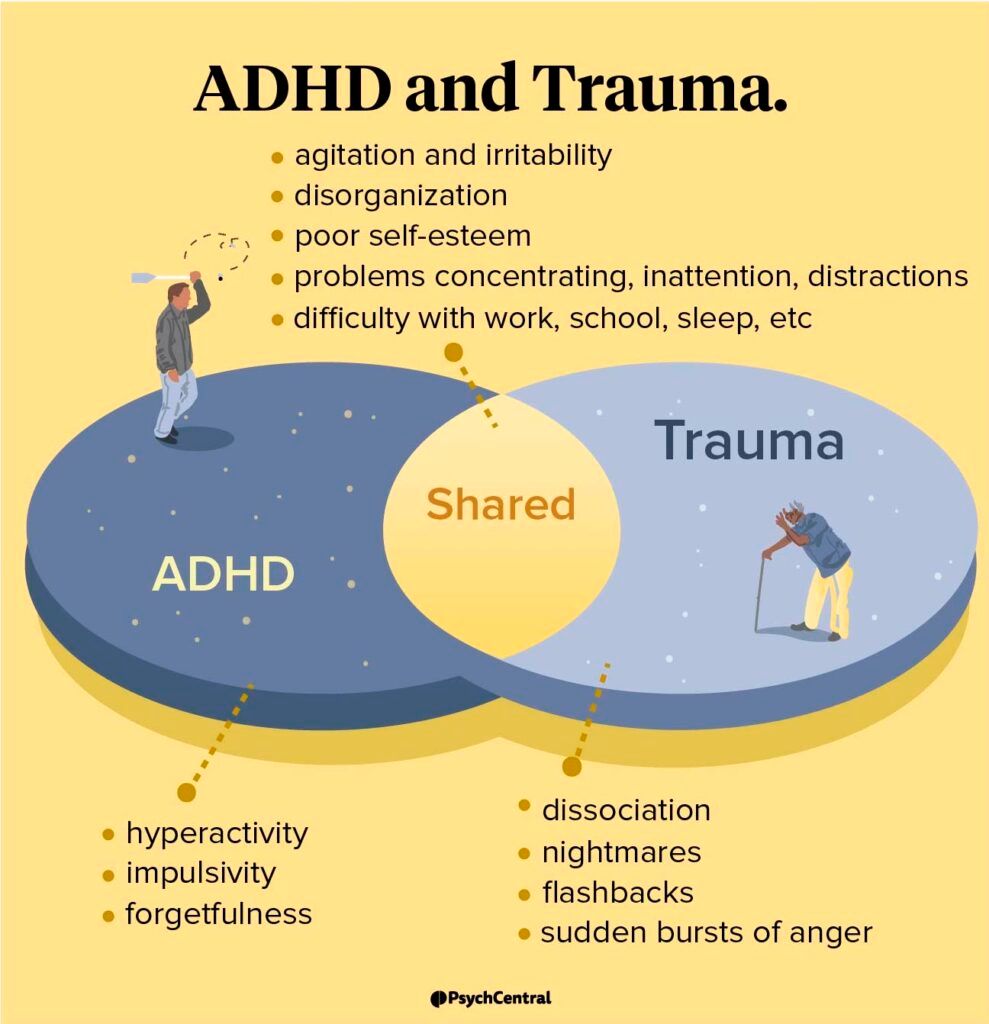
Sleep deprivation is a notorious moodswing trigger. Pulling an allnight study session or working rotating shifts can tip the scales. Likewise, chronic stress, major life changes, or unresolved trauma amplify risk. If you suspect trauma is affecting mood regulation, reading about childhood trauma ADHD can help clarify how early experiences influence mood and attention patterns.
Substance use
Alcohol, cannabis, and especially stimulants (like cocaine or ADHD meds taken without supervision) can provoke maniclike symptoms. Even caffeine in excess may exacerbate jitteriness during a hypomanic episode.
Psychological patterns
Perfectionism, rumination, or an allornothing mindset can make mood swings feel more extreme. Learning healthier coping strategies reduces the likelihood of escalation.
LowRisk vs. HighRisk Profile
| Factor | LowRisk | HighRisk |
|---|---|---|
| Family History | No firstdegree relative with bipolar | One or more firstdegree relatives with bipolar |
| Sleep Patterns | Regular 79h nightly | Frequent sleepless nights or erratic schedule |
| Substance Use | Minimal or none | Regular alcohol/cannabis/stimulant use |
| Stress Level | Managed, occasional stress | Chronic high stress or recent trauma |
How Diagnosis Works
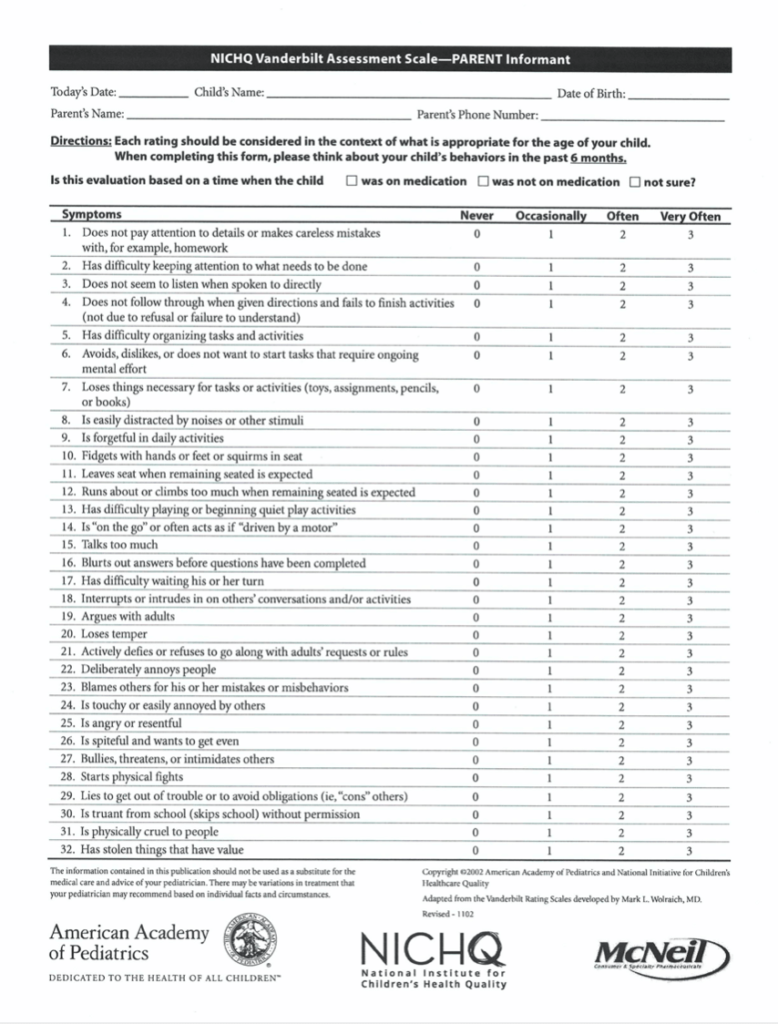
Screening tools you can try
A quick cyclothymia test (often found on reputable mentalhealth sites) asks about the frequency, duration, and impact of mood swings over the past two years. While not a substitute for a professional evaluation, it gives you a decent sense of where you stand.
Key DSM5 differences
The Diagnostic and Statistical Manual of Mental Disorders (DSM5) separates cyclothymia from bipolar primarily by:
- Number of episodes (cyclothymia requires numerous subthreshold episodes)
- Severity (symptoms must not meet full criteria for hypomania or major depression)
- Functional impact (cyclothymias impact is usually less disruptive)
When to seek a second opinion
If you receive conflicting resultssay, a therapist says you have cyclothymia while a psychiatrist leans toward bipolardont hesitate to ask for a referral or a second assessment. A clear diagnosis is the foundation for effective treatment.
Diagnostic flowchart (quick guide)
- Complete a reputable cyclothymia selfscreen.
- Consult a primary care physician or therapist.
- If symptoms are severe or unclear, get a referral to a psychiatrist.
- Psychiatrist conducts a full clinical interview + mood chart review.
- Diagnosis confirmed develop treatment plan.
Treatment & Lifestyle Tips
Therapy that works
Psychotherapy is often the first line of defense. CognitiveBehavioral Therapy (CBT) helps you recognize thought patterns that fuel mood swings, while Dialectical Behavior Therapy (DBT) adds skills for emotional regulation. Group psychoeducation sessions can also normalize your experience and connect you with peers.
Medication considerations
The question what is the best medication for cyclothymia? doesnt have a onesizefitsall answer. Many clinicians start with mood stabilisers such as lamotrigine or lowdose lithium. In some cases, atypical antipsychotics (e.g., quetiapine) are added if manic symptoms creep up. Antidepressants alone are usually avoided because they can trigger hypomanic spikes.
Everyday selfcare habits
- Sleep hygiene: Aim for 79hours, keep a regular bedtime, limit screens an hour before bed.
- Physical activity: Moderate exercise (walking, yoga) reduces stress hormones and stabilises mood.
- Mood tracking: Use a simple journal or an app to note sleep, energy, and emotions daily.
- Stress management: Mindfulness, breathing exercises, or even a hobby you love can buffer against triggers.
Cyclothymia and relationships
Partners often wonder how to support someone whose mood seems onandoff. Open communication is key. Share your feelings without blame (I feel worried when youre up all night), and agree on a plan for crisis moments (e.g., a trusted friend you can call).
Questions to ask your doctor
- Do my symptoms fit cyclothymia or bipolarII?
- Should I start a mood stabiliser now?
- What lifestyle changes will have the biggest impact?
- How often should I have followup appointments?
- Are there any redflag symptoms that require urgent care?
Helpful Resources List
These sites provide reliable, uptodate information and tools you can use right away:
- clear symptom checklists and treatment options.
- trustworthy medical perspective.
- practical advice for everyday living.
- Free moodtracking app suggestions (e.g., Moodpath, Daylio) pick one that feels intuitive.
- Support communities such as Bipolar UK forums connect with people who get it.
Conclusion
So, can cyclothymia become bipolar? The short answer is yes, but its far from inevitable. By staying alert to warning signs, understanding your personal risk factors, and embracing a balanced mix of therapy, medication (if needed), and healthy habits, you dramatically lower the odds of escalation. Remember, youre not alone on this journeytheres a wealth of professional guidance and community support waiting for you.
Whats your experience with mood swings? Have you found a strategy that helped keep things steady? Share your story in the comments or reach out with any questionsyou deserve answers that feel personal and empowering.
FAQs
Can cyclothymia develop into bipolar disorder?
Yes, research shows that between 10% to 50% of people with cyclothymia may eventually meet the criteria for Bipolar I or II disorder over time.
What are the early warning signs that cyclothymia is shifting to bipolar?
Signs include longer or more intense “high” periods, needing less sleep yet feeling wired, impulsive risky behavior, persistent and deepening depressive phases, and new significant stressors.
How does cyclothymia differ from bipolar disorder?
Cyclothymia involves milder and shorter mood swings with symptoms not severe enough to meet full mania or major depression criteria, while bipolar disorder features more severe manic or depressive episodes lasting weeks or months.
What factors increase the risk of cyclothymia becoming bipolar?
Key risk factors include a family history of bipolar disorder, frequent sleep disturbances, substance use, chronic or acute stress, and certain psychological patterns like perfectionism or rumination.
What treatment approaches help manage cyclothymia and prevent progression?
Effective management includes psychotherapy such as CBT and DBT, mood stabilizers like lithium or lamotrigine when needed, regular sleep and stress management, mood tracking, and avoiding substances that trigger mood swings.