Thrombocytopenia is the most common platelet problem youll see in people with chronic liver disease, and it usually shows up because the liver isnt making enough of the hormone that tells your bone marrow to make platelets, plus the spleen starts hoarding them. Below, well walk through why this happens, how you can spot it early, what you can actually do about it, and the pros and cons of each option all in a friendly, downtoearth style that feels like a chat over coffee.
Why Low Platelets?
What Links Cirrhosis and Low Platelets?
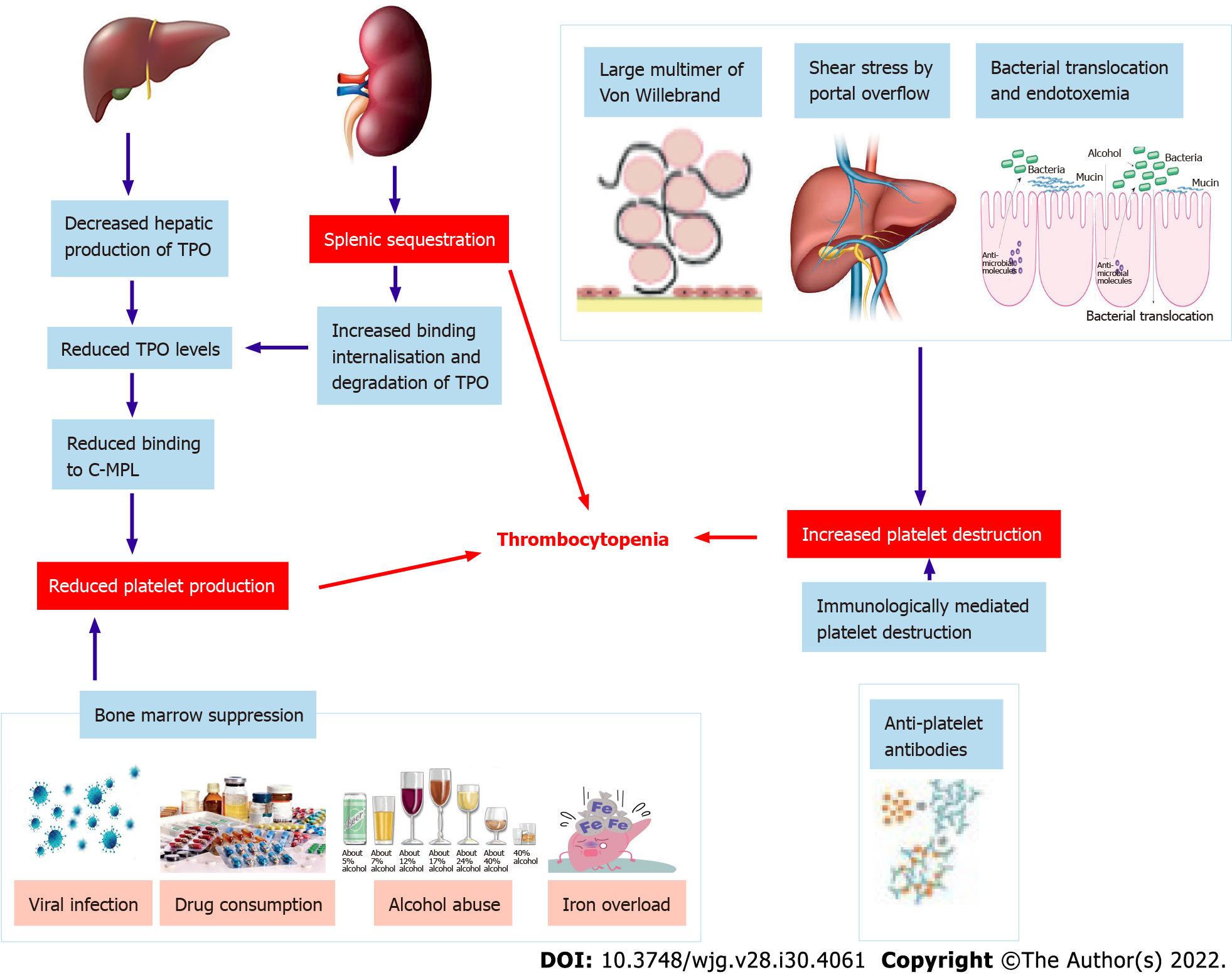
When the liver gets scarred thats cirrhosis it creates a traffic jam in the portal vein, the main highway that carries blood from the gut to the liver. This portal hypertension forces the spleen to enlarge (splenomegaly) and start gobbling up platelets like a vacuum cleaner. At the same time, the damaged liver cant produce enough thrombopoietin (TPO), the hormone that nudges the bone marrow to crank out fresh platelets. The double whammy drops the platelet count dramatically. For more detailed insights, the American Association for the Study of Liver Diseases provides comprehensive resources on this topic.
Key Mechanisms
- Splenic sequestration more platelets stuck in an enlarged spleen.
- Reduced TPO production the livers factory line slows down.
- Bonemarrow suppression in severe disease inflammation can blunt platelet production.
How Does Portal Hypertension Lead to Thrombocytopenia?
Think of portal hypertension as a pressure cooker. The higher pressure pushes blood into collateral vessels, including the spleens veins. The spleen swells, and its sinusoids (tiny blood channels) trap platelets, keeping them out of circulation. Studies show that up to 70% of patients with advanced portal hypertension have platelet counts below 150,000/L.
Data Snapshot
| Condition | Typical Platelet Range | Primary Cause |
|---|---|---|
| Compensated cirrhosis | 120180K | Early splenic sequestration |
| Decompensated cirrhosis | 70130K | Severe portal hypertension + TPO |
| Endstage liver disease | 50100K | Combined mechanisms |
Is Thrombocytopenia Always Present in EndStage Liver Disease?
No, not every patient hits the lowplatelet alarm. However, research from the American Association for the Study of Liver Diseases indicates that around 78% of individuals with ChildPugh class C cirrhosis experience platelet counts under 150,000/L. The severity of portal hypertension and the extent of liver dysfunction are the biggest predictors.
Why Do Some Patients Show High Platelets?
It sounds counterintuitive, but earlystage fibrosis or chronic inflammation can sometimes trigger a mild thrombocytosis. The liver releases inflammatory cytokines that temporarily boost platelet production, and iron overload (common in some liver patients) can also raise counts. Usually, though, high platelets are a fleeting phase before the spleen takes over.
Spotting Thrombocytopenia Early
What Are the Warning Signs?
Low platelets dont usually shout danger until theyre pretty low, but you can pick up subtle clues:
- Easy bruising or frequent nosebleeds.
- Bleeding gums when brushing.
- Prolonged bleeding from small cuts.
- Unexplained petechiae (tiny red dots) on the skin.
When Should You Get Tested?
If you have any form of chronic liver disease hepatitis, NAFLD, alcoholic liver disease, or an established cirrhosis diagnosis a complete blood count (CBC) every 36 months is a good habit. The lab will give you a platelet number, and you can compare it against these thresholds:
- Mild: 100150K
- Moderate: 50100K
- Severe: <50K (higher bleeding risk)
How Is It Coded?
For medical records, the ICD10 code D73.9 (Thrombocytopenia, unspecified) is commonly used when the cause is liver disease, though clinicians sometimes add a secondary code for the underlying liver condition (e.g., K74.60 for unspecified cirrhosis). Accurate coding helps ensure you get the right followup and insurance coverage for treatments.
RealWorld Example
Maria, 58, came in for her routine liver checkup after a year of managing hepatitis C. Her CBC showed a platelet count of 92,000/L. She felt fine but was surprised because she hadnt noticed any bruises. Her doctor explained the link to her portal hypertension and set up a monitoring plan, saving her from a potential surprise bleed before a scheduled liver biopsy.
Treatment Options Overview
What Are FirstLine Treatments?
If youre heading into a procedure or have a platelet count under 50,000/L, doctors usually start with platelet transfusions to boost the number quickly. However, transfusions are shortterm fixes and can lead to alloimmunization if used repeatedly.
Pharmacologic Boosters
- Eltrombopag an oral TPOreceptor agonist that can raise platelets by 3050K after 23 weeks.
- Avatrombopag approved specifically for patients with chronic liver disease undergoing invasive procedures.
- Both agents require monitoring for potential clotting complications.
Can Lifestyle Changes Help?
While lifestyle tweaks arent a magic wand, they can support your overall marrow health:
- Increase intake of vitaminB12, folate, and zinc essential for platelet formation.
- Stay clear of alcohol; even moderate drinking can worsen portal hypertension.
- Maintain a healthy weight; obesity fuels NAFLD, which can amplify liver injury and thrombocytopenia.
- Get vaccinated against hepatitis A and B to prevent further liver damage.
When Is Splenectomy Considered?
Removing the spleen (splenectomy) can dramatically improve platelet counts, but its a major surgery with notable risks infection, overwhelming postsplenectomy infection (OPSI), and postoperative portal pressure spikes. Modern practice reserves splenectomy for patients who are already surgical candidates for other reasons (e.g., variceal bleeding) or for those who fail medical therapy.
Emerging Therapies
Clinical trials are exploring geneediting approaches to boost TPO production directly within the liver. While still experimental, early results show promise of a lasting platelet increase without the need for ongoing drugs.
Specific Liver Conditions
Cirrhosis and Platelet Count
Cirrhosis is the poster child for low platelets. The enlarged spleen and low TPO combine to keep counts low, which can limit eligibility for liver transplantation or certain cancer therapies. Regular monitoring and early use of TPOagonists often keep patients above the 80,000/L threshold needed for most surgeries.
Liver Cancer (HCC) and Thrombocytopenia
Hepatocellular carcinoma (HCC) often coexists with cirrhosis, so low platelets become a doubleedged sword. Radiofrequency ablation or transarterial chemoembolization (TACE) requires a safe platelet level. If counts dip, physicians may pretreat with avatrombopag or a shortterm transfusion to avoid bleeding complications.
NAFLD and Early Platelet Trends
Nonalcoholic fatty liver disease can be silent, but studies have shown that a subtle rise in platelet count can precede the development of fibrosis. In other words, platelets can act as a early warning light a higher count in early NAFLD sometimes flips to a low count as fibrosis advances.
Acute Liver Failure
In sudden liver injury (e.g., acetaminophen overdose), platelets can plummet rapidly due to massive endothelial damage. Management focuses on stabilising the patient, often with plasma exchange and, when indicated, platelet transfusion to bridge the gap until the liver recovers or a transplant is arranged.
ConditionSpecific Table
| Condition | Platelet Trend | Key Management |
|---|---|---|
| Cirrhosis (advanced) | Decreasing | TPOagonist, monitor for variceal bleed |
| HCC with cirrhoshosis | Lowmoderate | Preprocedure transfusion or avatrombopag |
| NAFLD (early) | Slightly high low | Lifestyle, periodic CBC |
| Acute liver failure | Sharp drop | Urgent transfusion, consider transplant |
Balanced Risks and Benefits
Benefits of Treating Low Platelets
Raising platelet numbers can:
- Reduce spontaneous bleeding risk (e.g., GI bleeds).
- Make you a candidate for lifesaving procedures such as biopsies, surgeries, or transplant.
- Improve overall quality of life fewer bruises means less anxiety.
Potential Downsides
Every intervention carries a tradeoff:
- Platelet transfusions can trigger allergic reactions or develop antibodies that make future transfusions less effective.
- TPOagonists, while convenient, have been linked in rare cases to portal vein thrombosis a clot in the very vessel thats already under pressure.
- Splenectomy eliminates the spleens role in fighting certain bacteria, so lifelong vaccinations become essential.
Shared DecisionMaking Checklist
- Assess current platelet count and bleeding history.
- Identify upcoming procedures or surgeries.
- Discuss medication options, including sideeffects.
- Consider lifestyle modifications as adjuncts.
- Decide together on the timing of any invasive interventions.
Final Takeaways and Actions
Lets wrap up the big points:
- Root causes Portal hypertension squeezes platelets into an enlarged spleen, while a diseased liver cuts back on the hormone that tells bone marrow to produce more.
- Spotting it early Regular CBCs, awareness of bruising, and accurate ICD10 coding keep you ahead of complications.
- Treatment toolbox From platelet transfusions and TPOagonist pills to lifestyle tweaks and, in select cases, splenectomy, theres a spectrum of options tailored to severity.
- Balance matters Weigh the bleedingprevention benefits against potential clotting or infection risks, and involve your liver specialist in every decision.
Now its your turn. If youve been navigating low platelets alongside liver disease, what strategies have helped you feel safer? Have you tried a TPOagonist or found a diet tweak that made a difference? Drop a comment, share your story, or ask a question were all in this together, and your experience could be the lighthouse another reader needs.
FAQs
What causes thrombocytopenia in people with liver disease?
The main drivers are reduced production of thrombopoietin by the damaged liver and increased sequestration of platelets in an enlarged spleen caused by portal hypertension.
How is liver disease–related thrombocytopenia diagnosed?
Diagnosis starts with a routine complete blood count (CBC). If platelets are low, doctors assess liver function, imaging for splenomegaly, and may measure thrombopoietin levels to confirm the underlying mechanism.
When should treatment for low platelets be started?
Treatment is usually recommended when platelet counts fall below 50,000 µL, when a patient is scheduled for an invasive procedure, or if they have a history of bleeding.
What are the main treatment options for liver disease thrombocytopenia?
Options include platelet transfusions for rapid increase, oral TPO‑receptor agonists such as eltrombopag or avatrombopag, lifestyle measures (vitamins, alcohol avoidance), and, in selected cases, splenectomy.
Can lifestyle changes help improve platelet counts?
While they won’t replace medical therapy, a diet rich in vitamin B12, folate, and zinc, maintaining a healthy weight, and abstaining from alcohol can support overall marrow health and reduce further liver injury.