Whats new in the world of cervicalcancer staging? The 2024 FIGO update adds three subcategories to StageIB, creates a dedicated nodal StageIIIC, and finally folds highresolution imaging into the everyday classification. Why does that matter to you or a loved one? Because a more precise stage means a treatment plan thats tailored, less guesswork, and ultimately better chances for survival while avoiding unnecessary side effects.
Why Stay Current
Staging isnt just a number on a chartits the compass that guides every clinical decision. The newest FIGO revision reshapes surgical thresholds, radiotherapy fields, and systemictherapy choices. It also aligns global cancer registries, insurance coding, and research studies, making sure that the data we gather today will be comparable tomorrow. Most importantly, patients who understand their stage can ask sharper questions and feel more in control of their journey.
Staging at a Glance
Below is a quicklook table that captures the 2024 FIGO staging layout. Its designed for busy clinicians, medical students, and anyone who just wants the facts without a deep dive.
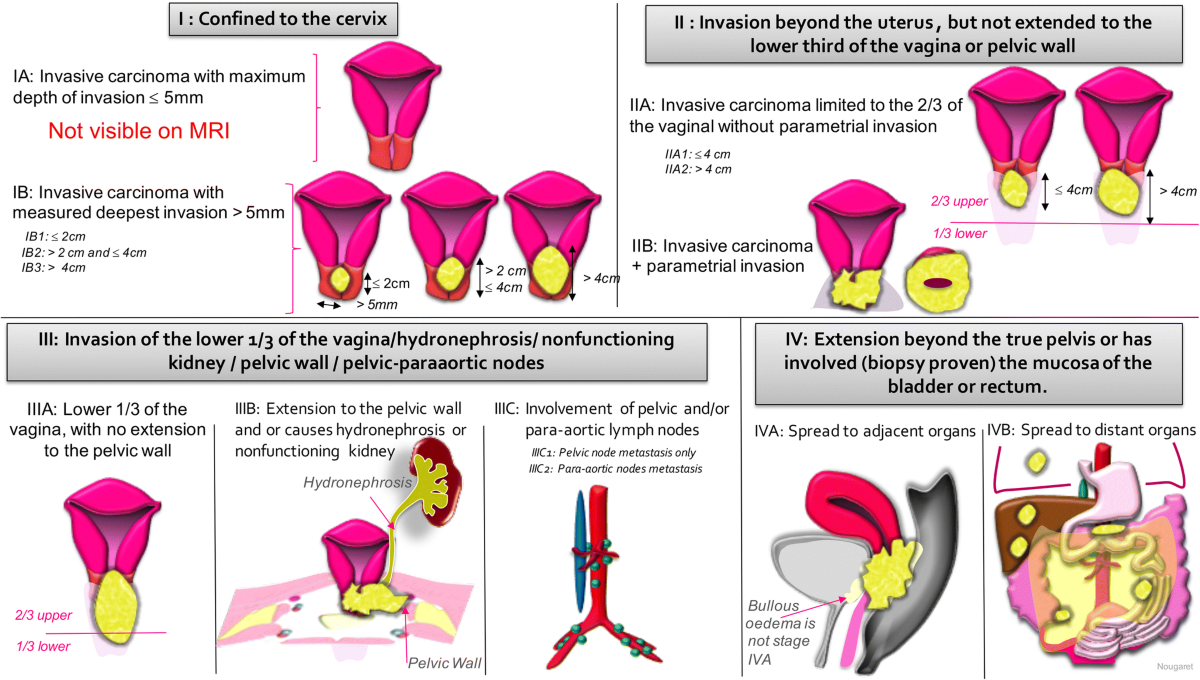
| Stage | Definition (2024 Update) |
|---|---|
| IA1 | Microscopic invasion 3mm depth, 7mm horizontal spread. |
| IA2 | Invasion >3mm but 5mm depth, 7mm width. |
| IB1 | Clinically visible lesion <2cm, no nodal disease. |
| IB2 | Lesion 2<4cm, no nodal disease. |
| IB3 | Lesion 4cm, no nodal disease. |
| IIA1 | Upper vaginal involvement <4cm. |
| IIA2 | Upper vaginal involvement 4cm. |
| IIB | Parametrial invasion on MRI. |
| IIIA | Lower third vaginal involvement <5mm. |
| IIIB | Pelvic sidewall extension or hydronephrosis. |
| IIIC1r | Pelvic lymphnode metastasis detected by imaging. |
| IIIC2r | Paraaortic lymphnode metastasis detected by imaging. |
| IVA | Invasion of bladder or rectum. |
| IVB | Distant metastases (lung, liver, bone, etc.). |
Notice the new r suffix? That signals a shift from purely clinical judgment to a hybrid model that welcomes MRI or PET/CT findings. If youre remembering the , youll see the same emphasis on imaging.
Mnemonic to Remember the SubStages
Many of us still love a good memory aid. Think of IBBig, IIInside, IIICheck nodes, IVBeyond. It reminds you that the larger the letter, the broader the disease spread, and the C in IIIC stands for Check nodes. Simple, right?
Imagings Role
Before 2018, FIGO staging was almost entirely clinical. The first hinted at imaging, but the 2024 update makes it mandatory for stages beyond IA. Heres why that matters.
Magnetic Resonance Imaging (MRI)
MRI is the gold standard for assessing tumor size to the nearest millimeter and for spotting parametrial invasionsomething a speculum exam can easily miss. Sensitivity for parametrial spread hovers around 85%, and the high contrast of soft tissue makes it invaluable when deciding between a simple conization and a radical hysterectomy.
CT & PET/CT for Nodes
When you suspect nodal disease, PET/CT lights up metabolic hotspots that CT alone cant catch. The new IIIC1r and IIIC2r categories exist solely because PET/CT can now reliably differentiate pelvic from paraaortic nodal spread. This distinction can change a surgical plan dramaticallysometimes sparing a patient from an extensive lymphnode dissection. For clinicians wanting to compare nodal staging with outcomes in other cancers (for example to discuss overall prognosis), resources on prostate cancer outlook may offer useful perspective on how nodal involvement influences treatment choices and expected trajectories.
Putting It All Together: A Practical Workflow
- 1 Clinical exam establish baseline and rule out obvious distant spread.
- 2 Pelvic MRI measure tumor dimensions, evaluate parametrial involvement.
- 3 PET/CT (if MRI suggests highrisk features or if you have palpable nodes) map pelvic and paraaortic nodes.
Following this sequence keeps you compliant with the latest FIGO rules and, more importantly, ensures youre not missing a hidden metastasis.
Pathology Insights
Even with dazzling imaging, the microscope still plays a starring roleespecially for stages IA and for evaluating lymphvascular space invasion (LVSI), a notorious predictor of recurrence.
Depth of Invasion & LVSI
IA substaging hinges on measuring depth in millimeters. A senior pathologist I once chatted with told me that an offbyamillimeter error can shift a patient from a simple cone biopsy to a radical hysterectomy. LVSI, on the other hand, isnt captured by imaging, yet its presence often nudges clinicians toward adjuvant chemoradiation.
When Pathology Beats Imaging
If a biopsy shows microinvasion that MRI cant see, the disease is still classified as IA. The 2024 FIGO guidelines explicitly state that pathology trumps imaging when the two disagreea useful safeguard against understaging.
Decision Tree: Pathology vs. Imaging
- Microscopic depth 5mm IA (pathology wins).
- Visible lesion 2cm on MRI IB (imaging wins).
- Node positive on PET/CT IIICr (imaging wins).
Top Patient Questions
Whats new in the latest FIGO staging?
The 2024 revision adds three IB subcategories (IB1IB3), introduces the nodal IIIC1r and IIIC2r stages, and officially incorporates MRI and PET/CT into the decisionmaking tree.
How does StageIIIC differ from older editions?
IIIC1r means pelvic lymphnode disease detected by imaging, while IIIC2r indicates paraaortic nodal spreadboth regardless of the primary tumors size.
Can I rely on a clinical exam alone?
Unfortunately, no. Imaging uncovers hidden parametrial invasion and nodal disease that a bimanual exam often misses, especially in larger tumors.
Is the mnemonic still valid for 2024?
Yesjust tack on C for Check nodes after III. So you get IAIBIIAIIBIIICIV.
What are the treatment implications of a new StageIB3?
Lesions 4cm typically steer clinicians toward concurrent chemoradiation rather than primary surgery, because the risk of positive margins increases sharply.
Benefits vs Risks
Every innovation carries a tradeoff. The biggest win of the new staging system is precision: patients get therapies that match their actual disease burden, which can improve survival and quality of life. The flip side? More advanced imaging means higher costs and, in some regions, limited access. Theres also a subtle phenomenon called stage creepwhere more sensitive tools upstage disease that would previously have been labeled lower, potentially leading to overtreatment.
Balance is key. If youre in a lowresource setting, discuss with your multidisciplinary team whether a highquality ultrasound and clinical exam can temporarily bridge the imaging gap while you arrange referral to a center with MRI capability.
RealWorld Story
Maria, a 55yearold from a rural clinic, first presented with a 3cm lesion on speculum. Her local doctor couldnt order an MRI, so she was slated for a radical hysterectomy. After a referral to a regional cancer center, an MRI showed parametrial invasionupgrading her to IIB. She then received chemoradiation, sparing her from an extensive surgery that would have carried higher morbidity. Marias case highlights why the newer FIGO staging is more than academicit can change a patients entire treatment journey.
Putting Staging Into Practice
Ready to adopt the 2024 FIGO system in your clinic or study group? Heres a stepbystep guide that even a busy resident can follow.
1 Update Protocols
Add MRI requisition forms for all lesions 2cm and PET/CT requisitions for any suspected nodal disease.
2 Train Your Team
Host a short workshopmaybe over coffeewhere you walk through the new table, discuss imaging pearls, and practice the mnemonic.
3 Integrate Into EMR
Create a staging checklist template that prompts clinicians to enter tumor size, parametrial status, and nodal findings. A dropdown menu for Stage can reduce errors.
4 Audit Outcomes
Every quarter, pull a report: How many patients were staged using imaging? What proportion were upstaged to IIIC? Correlate with treatment outcomes. This feedback loop reinforces adherence and highlights gaps.
Downloadable Resources
- PDF staging checklist (link to your clinics resource page).
- QR code for quick access to the full .
Trusted Sources
Building credibility starts with solid references. Below are the goto documents youll want on your desk (or bookmarked).
- FIGO 2024 Cervical Cancer Staging Guidelines the definitive source.
- Merck Manuals section on FIGO staging clear, patientfriendly language.
- American Cancer Societys How to Stage Cervical Cancer great for patient handouts.
- Radiology Society of North Americas 2018 FIGO paper explains the imaging evolution.
Whenever you quote these, link directly to the official PDFs or trusted medical sites. That not only fortifies your articles authority but also gives readers a path to verify the information.
Conclusion
The 2024 FIGO revision reshapes how we view cervical cancerfrom a blunt, mostly clinical label to a nuanced, imagingenhanced map of disease. By mastering the new subcategories, embracing MRI and PET/CT, and respecting the indispensable role of pathology, clinicians can craft treatment plans that are both aggressive enough to win the battle and gentle enough to preserve quality of life. If youve read this far, you already have a solid foundationnow its time to put it into practice, discuss it with your care team, and, if youre a patient or caregiver, ask the right questions at your next appointment.
Whats your experience with the latest FIGO staging? Have you noticed a difference in treatment decisions in your practice or personal journey? Share your thoughts in the comments below, and lets keep the conversation going. If you have questions, dont hesitate to askknowledge is power, and together were stronger.
FAQs
What are the major changes in the latest FIGO staging of cervical cancer?
The 2024 FIGO update introduces three subcategories within Stage IB, defines nodal Stage IIIC with IIIC1-r (pelvic nodes) and IIIC2-r (para-aortic nodes), and mandates the use of imaging (MRI and PET/CT) beyond Stage IA for more accurate staging.
How does the new Stage IIIC classification affect treatment?
Stage IIIC now explicitly includes lymph node metastasis detected by imaging, directing patients to chemoradiation and helping tailor radiation fields, potentially avoiding extensive lymph node dissection when para-aortic nodes are not involved.
Why is imaging essential in the 2024 FIGO cervical cancer staging?
Imaging, particularly MRI and PET/CT, provides precise tumor size measurement, detection of parametrial invasion, and nodal metastases, reducing understaging common with clinical exams alone and enabling more accurate treatment decisions.
When does pathology override imaging in staging decisions?
Pathology findings take precedence in cases of microscopic disease, such as microinvasion ≤5 mm depth (Stage IA), even if imaging suggests a higher stage—this prevents overstaging and inappropriate treatment escalation.
What mnemonic helps remember the FIGO 2024 cervical cancer sub-stages?
“IB-Big, II-Inside, III-Check nodes, IV-Beyond” is used, with the added “C” in IIIC reminding clinicians to check for nodal involvement for accurate staging and treatment planning.