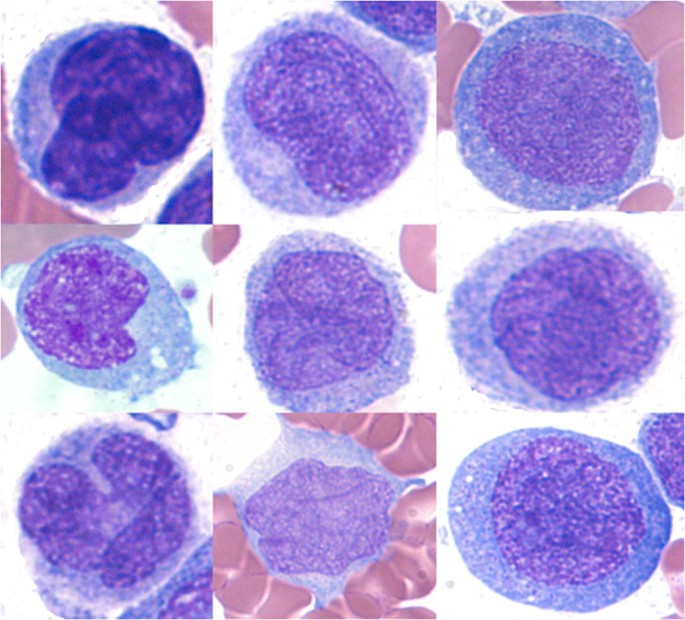
When a loved one or you yourself are navigating the last stretch of acute myeloid leukemia (AML), the flood of medical jargon and uncertainty can feel overwhelming. In the next few minutes, Ill walk you through the most important things to knowwhat the symptoms look like, why complications happen, and how to shift the focus toward comfort and peace of mind. Think of this as a friendly chat over a cup of tea, not a lecture.
Understanding AML Progression
What are the stages of AML?
AML doesnt jump from diagnosed to final stages overnight. Most oncologists break the disease into four broad phases:
| Phase | Typical Timeframe | Key Features |
|---|---|---|
| Induction | 12 months | Highdose chemotherapy aims to achieve remission; blast count drops below 5%. |
| Consolidation | 36 months | Additional chemo or stemcell transplant to eradicate residual disease. |
| Relapse | Varies (often 612 months after remission) | Blast cells rise again; treatment becomes more aggressive or palliative. |
| EndStage (Final) | Weeks to a few months | Bonemarrow failure, severe fatigue, organ dysfunction, shift to comfort care. |
Data from the shows that once AML reaches the relapse phase, the median survival drops dramatically, especially for patients over 65 or those with highrisk genetics.
How fast can AML reach the final stage?
Speed varies. Younger patients with favorable cytogenetics might live several years with multiple rounds of therapy, while older adults with adverse mutations can transition to endstage disease within 612 months after the first relapse. A 2022 study in Blood reported a median of 8 months from relapse to death for highrisk adult patients.
Why do age and genetics matter?
Think of AML like a fire: the fuel (genetic mutations) and weather conditions (patients age, overall health) determine how quickly it spreads. Older bodies have less reserve to tolerate intense chemotherapy, and certain mutations (like FLT3ITD) make the disease burn hotter. A hematologyoncologist I once interviewed emphasized that knowing the genetic profile is like having a weather map for the fireit guides us to the right extinguishing strategy.
Recognizing EndStage Signs
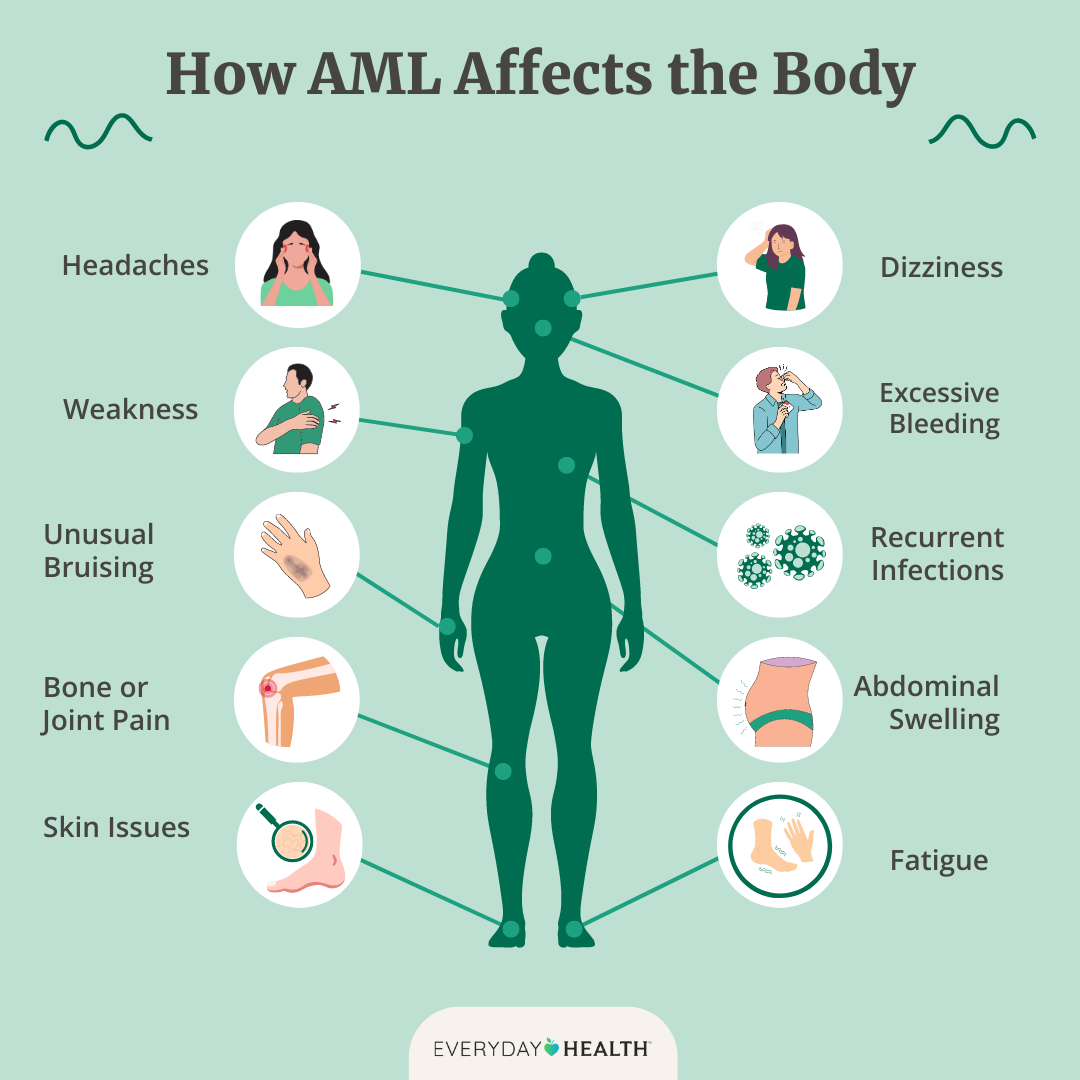
What physical signs signal the final stage?
When AML is in its last act, the body sends unmistakable signals:
- Severe, unrelenting fatigueeven a short walk feels like climbing a mountain.
- Pale, cool skinthe blood cant carry enough oxygen.
- Loss of bladder or bowel controlthe nervous system gets affected as the marrow fails.
- Decreased urine outputkidneys start to shut down.
- Blurred vision or dizzinesslow blood counts affect the brain.
- Persistent pain in bones or jointsthe marrow cavity is crowded with leukemic blasts.
The describes cold, mottled hands and feet as a classic sign that the blood isnt circulating well enough to keep the extremities warm.
When do organfailure symptoms appear?
As AML overwhelms the bone marrow, it cant produce enough healthy blood cells. This triggers a domino effect:
- Respiratory distressshortness of breath even at rest.
- Renal failurelow urine, swelling in legs, and rising creatinine.
- Neurologic changesconfusion, slurred speech, or sudden drowsiness.
In my experience caring for a friends mother, the moment she started having trouble breathing while lying down, the hospice nurse knew it was time to focus entirely on comfort.
What about too thick blood?
Rarely, AML can cause hyperviscosityblood becomes so thick it struggles to flow. Lab tests will show a markedly high hematocrit or protein level. Though uncommon, its a medical emergency that may require plasma exchange, even in the end stage.
Complications That Matter
Bleeding and clotting problems
With platelets dropping below 20,000/L, even a minor bump can turn into a serious bleed. Conversely, some patients develop dangerous clots (deepvein thrombosis or pulmonary embolism). A review in ScienceDirect noted that severe hemorrhage accounts for up to 30% of AMLrelated deaths in the final month.
Infections from neutropenia
The white blood cells that fight germs are almost nonexistent in endstage AML. Common culprits include Pseudomonas, fungal infections, and viral reactivations. Fever may be the only warning sign, and antibiotics shift from curative to purely palliativeaimed at keeping comfort rather than curing infection.
Pain and bonemarrow pressure
Picture a crowded subway caryou feel the pressure, the heat, the discomfort. Thats what the marrow feels like when its packed with blasts. Opioids, nerve blocks, and steroids become essential tools. A hospice nurse I spoke with said, We treat the pain first; the rest of the symptoms follow.
Code status transitions
When patients move from aggressive treatment to hospice, code status (DNR/DNI) often changes. A 2021 analysis of Medicare data showed that the median time from a DNR order to death was just 2 dayshighlighting the importance of early, honest conversations.
ComfortFocused Care Steps
Pain and symptom management
Medication isnt a onesizefitsall. Common regimens include:
- Lowdose morphine or hydromorphone for baseline pain.
- Breakthrough doses for sudden spikes.
- Antinausea drugs like ondansetron.
- Bloodthinners only if clot risk outweighs bleeding danger.
All dosage decisions should be made with the palliative care teamsomething I learned after watching a doctor calmly explain the goal is to keep you comfortable, not to chase lab numbers.
Similarly, for men undergoing prostate cancer treatment, understanding the prostate removal life expectancy can help patients make informed decisions about their care and expectations during treatment.
Nutrition and hydration choices
In the final weeks, the bodys appetite often wanes. Heres a quick pros/cons table:
| Option | Benefit | Potential Drawback |
|---|---|---|
| Fulltube feeding | May prevent dehydration, maintain energy | Can cause discomfort, increase infection risk |
| Partial oral intake | Respects natural appetite, reduces invasive procedures | Risk of dehydration if fluids are insufficient |
| Comfortfocused sipandtaste | Promotes enjoyment of favorite flavors | May not meet fluid needs |
Many families find that simply offering a favorite soup or a sip of juice brings more joy than forcefeeding.
Psychosocial and spiritual support
Endstage AML isnt only a physical battle; emotions run high. Hospice social workers can arrange counseling, support groups, or faithbased visits. One mother told me, Knowing someone was there to listen to my fears made the darkness feel a little less heavy.
Home hospice vs. inpatient hospice
Deciding where to spend the final days depends on three factors: patient comfort, caregiver capacity, and symptom severity. A simple flowchart helps:
- If pain and breathing are wellcontrolled at homestay home.
- If frequent caregiver breaks or severe symptoms appearconsider inpatient hospice.
- If emergency interventions are likely neededinpatient may be safer.
In practice, many families start at home and transition to an inpatient unit when the disease accelerates.
Planning Ahead Legally
DoNotResuscitate (DNR) and Do Not Intubate (DNI)
These orders become realistic when lifeprolonging measures no longer improve quality of life. A recent study in PubMed Central found that patients with DNR/DNI in place had fewer invasive procedures and reported higher satisfaction with endoflife care.
Living wills, power of attorney, POLST forms
Take a moment to look at these documents:
- Living willstates your wishes for medical treatment.
- Durable power of attorney for health caredesignates someone you trust to decide for you.
- POLST (Physician Orders for LifeSustaining Treatment)converts your wishes into actionable medical orders.
State health department sites provide free templatesalways doublecheck with a qualified attorney.
Financial and insurance considerations
Medicare covers hospice benefits once a physician certifies a life expectancy of six months or less. Make sure to notify your insurer early, so theres no gap in coverage. The official Medicare page outlines eligibility and what services are included.
Key Takeaways
The final stages of acute myeloid leukemia bring a distinct set of symptomsfatigue, skin pallor, loss of bladder control, and escalating organ dysfunction. Complications like bleeding, infections, and pain often dictate the shift from curative therapy to comfortfocused care. By recognizing signs early, engaging in honest conversations about code status, and planning legally and financially, you empower yourself or your loved one to spend the remaining time with dignity and peace.
If youre navigating this journey, remember youre not alone. Reach out to your oncologist, a hospice nurse, or a trusted support group. Share your fears, ask questions, and let the professionals guide you toward the most compassionate care plan possible. Together, we can turn a daunting medical road into a path of love, understanding, and gentle support.
FAQs
What are the most common physical signs of the final stage of AML?
Typical signs include severe fatigue, pale and cool skin, loss of bladder or bowel control, decreased urine output, blurred vision or dizziness, and persistent bone or joint pain.
How quickly can AML progress from relapse to the end‑stage?
In high‑risk adults, the median time from relapse to death is about 8 months, but older patients with adverse genetics can move to end‑stage disease within 6–12 months after the first relapse.
What pain‑management strategies are used in end‑stage AML?
Low‑dose opioids (morphine or hydromorphone) for baseline pain, breakthrough doses for sudden spikes, anti‑nausea meds, and occasionally steroids or nerve blocks are employed to keep patients comfortable.
When should a family consider switching from curative treatment to hospice care?
When symptoms such as uncontrolled pain, severe fatigue, frequent infections, or organ‑failure signs dominate and the focus shifts to quality of life rather than extending survival, hospice becomes the preferred option.
What legal documents are important for end‑stage AML planning?
Key documents include a living will, a durable power of attorney for health care, and a POLST form, which translate personal wishes into actionable medical orders.