Short answer: most people see their symptoms fade within a few months, but a smallsize slice of patients end up with longlasting joint problems, so the condition isnt automatically permanent.
Why does this matter? Knowing the typical timeline helps you plan treatment, set realistic expectations, and avoid unnecessary worry.
Quick Answer Summary
In rheumatology, permanent usually means the disease persists beyond a year and requires ongoing medication. For reactive arthritis, about 6070% of folks experience full remission in under six months, roughly 2030% have intermittent flareups, and only 510% develop chronic arthritis that sticks around for years.
| Outcome | % of Patients | Typical Duration | Common Followup |
|---|---|---|---|
| Full remission | 6070% | 36months | No further therapy needed |
| Intermittent flareups | 2030% | 6months2years | NSAIDs, physical therapy |
| Chronic arthritis | 510% | >12months | DMARDs or biologics |
These numbers come from data compiled by institutions such as and the . The takeaway? Most of us wont be battling this forever, but staying informed can make a huge difference.
Usual Disease Duration
If youve just been told you have reactive arthritis, the first thing you probably wonder is, How long will this last? In most cases, the disease runs its course in three to twelve months. The Cleveland Clinic notes that the median duration is around six months, with many patients feeling completely back to normal after a short burst of joint pain.
When symptoms linger past the sixmonth mark, its a signal to keep a closer eye on things. The National Center for Biotechnology Informations StatPearls article points out that persistent joint swelling beyond six months raises the odds of a chronic trajectory.
Factors that can stretch the timeline include:
- Older age at onset
- A bacterial trigger that was especially aggressive (think Salmonella or Shigella)
- Carrying the HLAB27 gene, which makes the immune system more likely to stay on alert
Causes of FlareUps
Even after the initial infection clears, some people experience a second wave of pain. Why does the immune system decide to strike again?
First, reactive arthritis is more of an autoinflammatory reaction than a classic autoimmune disease. The immune system gets a brief glimpse of the offending microbe, forms a memory, and sometimes keeps the fire lit for longer than necessary.
New infections, stress, hormonal shifts, or even certain medications can reignite the flare. A handful of recent case reports have also linked COVID19 to postviral reactive arthritis, showing that the virus can serve as a fresh trigger in susceptible individuals.
Consider the story of Maya, a 32yearold teacher who recovered from a mild COVID19 infection in early 2024. Six weeks later, she woke up with swollen knees and a lowgrade fever. Her rheumatologist explained that the virus likely sparked a reactive arthritis episodean example of how the condition can resurface long after the original bug.
Reactive vs Rheumatoid
Its easy to mix up reactive arthritis with rheumatoid arthritis, especially when both involve painful joints. Heres a quick sidebyside look:
| Feature | Reactive Arthritis | Rheumatoid Arthritis |
|---|---|---|
| Typical Trigger | Recent bacterial or viral infection | Autoimmune mechanisms (no infection) |
| Common Joints | Knees, ankles, toes (asymmetrical) | Hands, wrists, feet (symmetrical) |
| Lab Findings | Often HLAB27+, RFnegative | RF+, antiCCP+, often elevated ESR/CRP |
| Course | Selflimited in most cases | Chronic, progressive |
Notice the differences? Reactive arthritis typically shows up after a GI or genitourinary infection, hits the lower extremities, and often resolves on its own. Rheumatoid arthritis, on the other hand, is a longterm systemic disease that needs aggressive, ongoing treatment.
Root Causes Explained
Lets break down the main culprits behind reactive arthritis:
- Bacterial triggers: The classic offenders are Chlamydia trachomatis, Salmonella, Shigella, Yersinia, and Campylobacter. These bugs invade the gut or urogenital tract, and the immune system occasionally misfires, targeting the joints.
- Viral triggers: While less common, virusesincluding the recent SARSCoV2have been implicated in case series that describe joint inflammation appearing weeks after the respiratory illness.
- Genetic susceptibility: Carrying the HLAB27 gene doesnt guarantee youll develop the condition, but it does raise the odds dramatically. Roughly 7080% of people with reactive arthritis are HLAB27 positive.
Think of it like a security system that gets overexcited after a breakin. The alarm (immune response) is meant to protect you, but sometimes it keeps ringing even after the intruder is gone.
Diagnosis Process Overview
Getting a diagnosis isnt a wild guessits a stepbystep puzzle. Your doctor will look for three key pieces:
- History of a recent infection: A GI bug or a chlamydia episode within the past month or two.
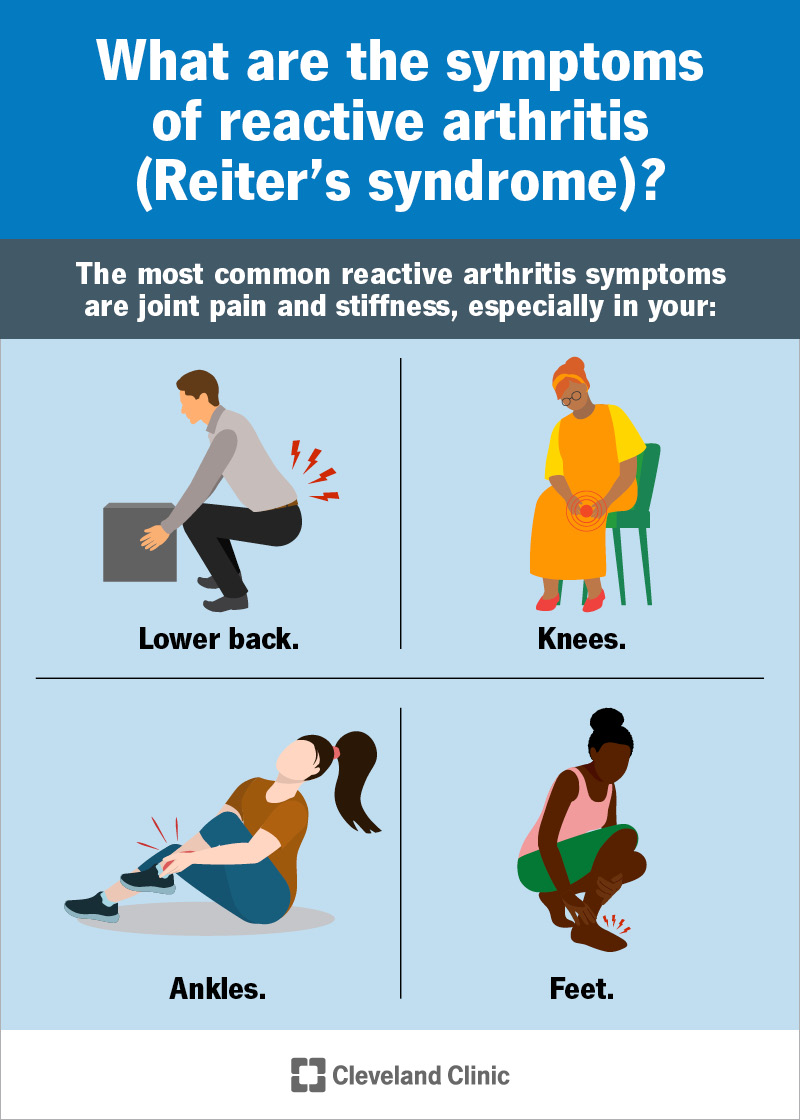
- Joint symptoms: Swelling, pain, and sometimes redness in one or a few joints (often the knees, ankles, or feet).
- Exclusion of other rheumatic diseases: Blood tests to rule out rheumatoid factor, antiCCP, and other markers.
Typical lab work includes CBC, ESR/CRP, urine or stool cultures (if a bacterial source is suspected), and an HLAB27 test. Imaginglike an Xray, ultrasound, or MRIhelps visualize joint effusion and rule out damage that would suggest a different arthritis.
The provides a handy flowchart for clinicians, but the important part for you is knowing what questions to expect and why each test matters.
Treatment Options Guide
Good news: most treatment plans start simple and only get more intense if needed.
Firstline: NSAIDs & Rest
Nonsteroidal antiinflammatory drugs (like ibuprofen or naproxen) are usually the first line to knock down pain and swelling. Pair them with plenty of rest for the affected jointthink ice, elevate, and a short break from heavy walking.
Shortterm Steroids
If NSAIDs arent enough, a short burst of oral prednisone can calm the inflammation quickly. The key is to taper the dose over a few weeks to avoid longterm side effects.
When to Consider DMARDs
For the 510% who develop chronic arthritis, diseasemodifying antirheumatic drugs (DMARDs) such as sulfasalazine or methotrexate become the mainstay. In some refractory cases, biologics like TNFinhibitors may be prescribed.
Physical Therapy & Lifestyle
Gentle rangeofmotion exercises keep joints supple and help prevent stiffness. A physiotherapist can design a program that respects your pain levels while strengthening surrounding muscles.
Tracking Your Flares
Keeping a simple log can be eyeopening. Write down the date, joint(s) affected, any potential triggers (like a new infection or stress), and what treatment helped. Over time youll spot patterns, and your doctor will have concrete data to finetune therapy.
Living With It
Now, lets talk about the daytoday reality. Heres a short, anonymized story that might feel familiar:
James, a 45yearold construction manager, got a nasty bout of food poisoning from undercooked fish. Two weeks later, his knees were swollen and he felt a burning sensation in his eyes. After a rheumatology visit, he learned he had reactive arthritis. With NSAIDs, a brief steroid tap, and a dedicated physicaltherapy routine, his symptoms faded in four months. He now watches his diet, stays up to date on vaccinations, and keeps a flare notebooka habit that helped him catch a mild recurrence early.
Practical tips for anyone navigating this condition:
- Choose supportive footwearthink cushioned sneakers or orthotic inserts.
- Take short, frequent breaks if you have a sedentary job; a fiveminute walk every hour can keep joints from locking up.
- Stay hydrated and maintain a balanced diet rich in omega3 fatty acidsthese may help reduce overall inflammation.
- Know the redflag signs that warrant urgent care: sudden high fever, rapidly worsening swelling, or new skin lesions.
- Connect with reputable resources: the , , and the Arthritis Foundation all offer trustworthy guidance and community support.
Conclusion
In a nutshell, reactive arthritis most often follows a brief, infectiontriggered course that resolves within months. Only a minority experience persistent, chronic joint pain, and those cases can be managed with targeted therapies. By staying informed, watching for flare triggers, and working closely with a rheumatologist, you can dramatically lower the odds of a permanent outcome.
Got questions about your own symptoms, or want to share a story of how you dealt with a flare? Drop a comment belowyour experience could help someone else navigating the same road. And remember, youre not alone; theres a whole community ready to support you.
FAQs
Can reactive arthritis become permanent?
Most cases of reactive arthritis are not permanent and resolve within months, but a small percentage of people develop chronic joint problems that last longer.
How long does reactive arthritis usually last?
Reactive arthritis typically lasts 3 to 6 months, with most people recovering fully. Symptoms lasting beyond 6 months may indicate a chronic form.
What causes reactive arthritis to become chronic?
Factors like HLA-B27 gene, severe initial infection, and lack of response to NSAIDs increase the risk of chronic reactive arthritis.
Is there a cure for reactive arthritis?
There is no specific cure, but most cases resolve on their own. Chronic cases may require ongoing treatment to manage symptoms.
Can reactive arthritis come back after it goes away?
Yes, some people experience flare-ups or recurrences, especially if they have the HLA-B27 gene or are exposed to new infections.