Understanding Airway Remodeling
What is airway remodeling in asthma?
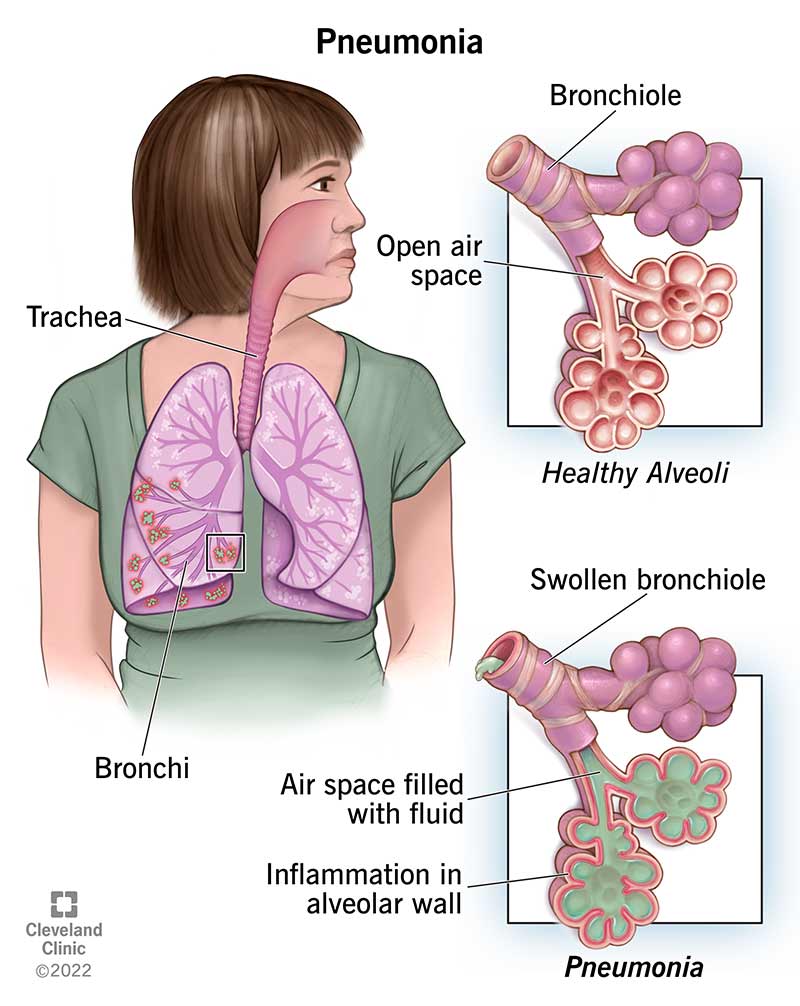
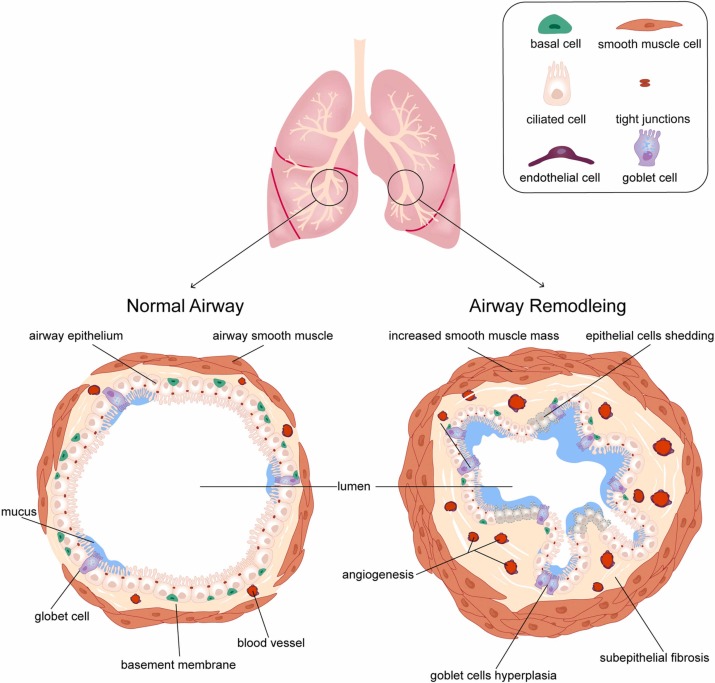
Airway remodeling is the lungs way of rebuilding itself after prolonged inflammation. Think of it like a garden thats been overwatered for months: the soil (the airway walls) thickens, new weeds (smoothmuscle cells) sprout, and the pathways become harder to walk through. In asthma, this means a thicker basement membrane, larger smoothmuscle bundles, more mucusproducing glands, and even tiny scarlike deposits.
Why does remodeling happen?
It starts with chronic inflammation. Cytokinestiny messenger proteins released by immune cellssignal the airway lining to grow and change. Over time, repeated exposure to allergens, pollutants, cigarette smoke, or viral infections fuels this cycle. Genetic predisposition can also make some peoples airways more remodelprone. In short, the lungs are trying to protect themselves, but the protection ends up narrowing the airway highway.
Cellular players the epithelium on the edge of a new era
Recent research titled Airway remodeling in asthma and the epithelium: on the edge of a new era highlights how the epithelial cells (the lining of the airway) act as both sentinels and architects. When theyre stressed, they release growth factors that accelerate remodeling. Understanding this layer is why new biologic therapies are aiming at the epithelium itself, not just the inflammation.
Airway remodeling vs. normal obstruction
Most people think of asthma as bronchoconstrictionthe muscles around the airway tighten temporarily. Thats a reversible squeeze. Remodeling, on the other hand, is a structural change; its like renovating the hallway so its permanently narrower. Even if you use a quickacting inhaler, the underlying remodeling may still limit airflow.
Is Remodeling Reversible?
What does the latest research say?
According to a 2025 , mild asthma patients who start highdose inhaled corticosteroids (ICS) early can see up to a 3040% reduction in airway wall thickness after two years. In severe, longstanding cases, the same studies report only modest improvements, suggesting that the changes become largely permanent.
Clinical data: mild vs. severe asthma
| Severity | Typical Reversibility | Measurement Methods |
|---|---|---|
| Mild, earlystage | 3040% reduction in wall thickness | CT densitometry, spirometry (FEV improvement) |
| Moderate | 1020% improvement | Bronchoscopy biopsy, FeNO levels |
| Severe, chronic | 5% change (often none) | Highresolution CT, longterm lungfunction decline |
Factors that boost chances of reversal
- Early diagnosis: The sooner you control inflammation, the less building occurs.
- Adherence to therapy: Skipping doses gives inflammation a chance to run wild.
- Targeted biologics: AntiIL5, antiIL4R agents have shown modest wallthickness reductions.
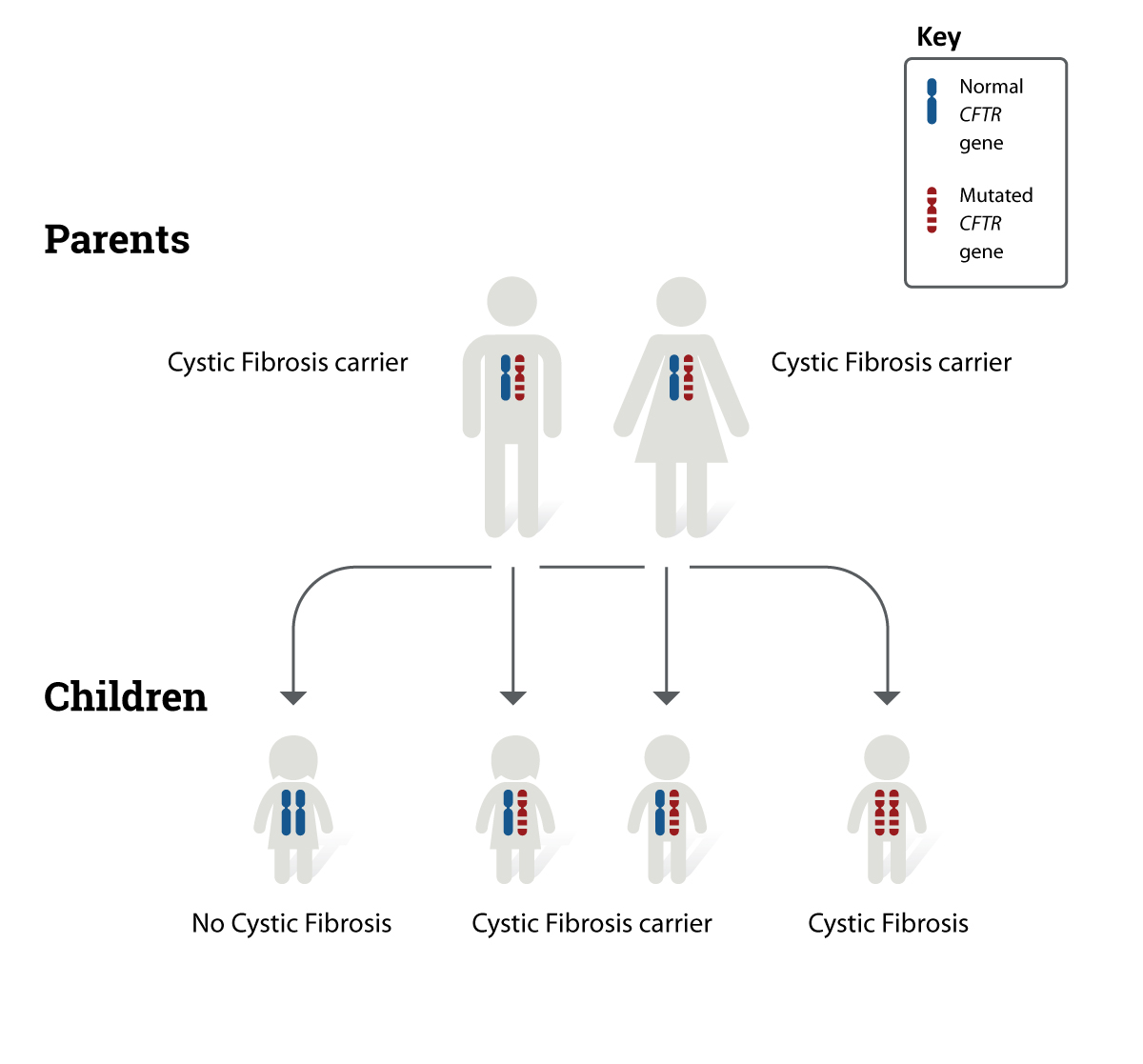
- Lifestyle control: Avoiding smoke, pollutants, and allergens reduces the stimulus for remodeling. For people with coexisting conditions such as cystic fibrosis, paying attention to respiratory safety and relationships that support treatment adherence can be especially helpful; see guidance on cystic fibrosis safety for practical tips on reducing household and environmental risks.
When reversal is unlikely what permanent really means
If remodeling reaches a point where scar tissue dominates, the airway loss is irreversible. This can shorten airway remodeling life expectancy in the sense that lungfunction trajectories decline faster, leading to more frequent exacerbations and, over decades, a modest impact on overall lifespan. The key is that permanent isnt a life sentence; it just means youll need to focus on managing the remaining function.
Treatments That Help
Pharmacologic options
Inhaled corticosteroids (ICS) remain the cornerstone. They dampen inflammation, giving the airway a chance to heal. Highdose regimens, especially when started early, have the strongest evidence for reversing wall thickening.
Biologics such as mepolizumab (antiIL5) or dupilumab (antiIL4R) are newer players. Clinical trials report modest improvements in airway thickness and, more importantly, fewer exacerbationsboth of which indirectly support remodeling reversal.
Bronchial thermoplasty uses controlled heat to reduce smoothmuscle mass. Results are mixed; some patients report lasting symptom relief, while others see little structural change. Its usually reserved for severe asthma that isnt controlled by medication.
Nonpharmacologic strategies
- Trigger control: Reduce exposure to dust mites, pet dander, seasonal pollen, and especially tobacco smoke.
- Exercise: Regular aerobic activity improves airway clearance and can modestly lower inflammation.
- Weight management: Excess weight adds mechanical pressure on the chest and raises inflammatory markers.
- Breathing techniques: Strategies like the Buteyko method or diaphragmatic breathing can lessen hyperresponsiveness.
Monitoring progress
Keeping an eye on your lungs is essential. Spirometry every 36 months tells you if FEV is holding steady or slipping. Fractional exhaled nitric oxide (FeNO) gives a snapshot of airway inflammation. For the truly curious (or those under specialist care), highresolution CT scans can directly visualize wall thickness over time.
Sample monitoring schedule
Quarterly: Spirometry and symptom diary.
Biannual: FeNO measurement.
Every 23 years: Lowdose CT to track structural changes.
Remodeling in Other Conditions
Airway remodeling in COPD
Chronic obstructive pulmonary disease (COPD) also features airway remodeling, but the patterns differ. COPDs remodeling is driven more by smokingrelated inflammation and emphysematous destruction, leading to a loss of elastic recoil rather than the thickening seen in asthma. Still, some therapies that work for asthmalike inhaled steroidscan modestly slow COPD remodeling, especially in patients with the asthmaCOPD overlap phenotype.
Overlap syndromes
When asthma and COPD coexist, the airway walls can become a chaotic mix of thickening, mucus hypersecretion, and loss of elasticity. In these cases, reversibility is even harder to achieve, underscoring the importance of early, aggressive control of any inflammatory component.
Personal Stories & Lessons
Case study A A 28yearold with mild asthma
Emily was diagnosed at 12, started on lowdose ICS, and was just okay through her teens. At 25 she began experiencing more wheeze and visited a pulmonologist who escalated her therapy to highdose inhaled steroids plus a shortcourse of oral steroids. Over the next 24 months, her CT scans showed a 35% reduction in airway wall thickness, and her FEV improved by 12%. Emilys story illustrates that early, consistent treatment can indeed shrink the structural changes.
Case study B A 55yearold with severe asthma
James struggled with asthma since childhood, but he stopped his medication after his teens, thinking he was cured. By his forties he was on daily oral steroids, still coughing, and his lung function had plummeted. Even after starting biologics, his CT scans showed only a 4% change in wall thickness. James experience reminds us that once remodeling reaches a certain depth, the reversible window closes, and the focus shifts to preservation.
Patient tip roundup
- Keep a symptom diary youll spot patterns that help you avoid triggers.
- Never skip a controller inhaler dose; its the backbone of any reversal plan.
- Ask your doctor about biologic eligibility if you have frequent exacerbations.
- Invest in a good air purifier at home; cleaner air = less inflammation.
- Stay active a 30minute walk most days can make a measurable difference.
Conclusion
So, is airway remodeling reversible? The short answer is: yes, partially, and mostly when you act early and stick to a solid treatment plan. In mild or newly diagnosed asthma, aggressive antiinflammatory therapy can shrink the airway walls and improve breathing. In chronic severe cases, the changes tend to stay, meaning youll need to concentrate on managing the remaining function and preventing further damage.
The good news is that you have tools at your disposalhighdose inhaled steroids, cuttingedge biologics, lifestyle tweaks, and regular monitoringall aimed at giving your lungs the best chance to heal. Talk to your healthcare provider about a personalized plan, stay consistent, and remember that every breath you protect today helps you breathe easier tomorrow.
FAQs
What is airway remodeling in asthma?
Airway remodeling refers to structural changes in the airways caused by prolonged inflammation, including thickened airway walls, increased smooth muscle mass, more mucus glands, and scar-like deposits, which narrow the airways permanently.
Can airway remodeling be reversed with treatment?
Yes, airway remodeling can be partially reversible, particularly in mild or early-stage asthma. High-dose inhaled corticosteroids started early may reduce airway wall thickness by 30–40%, while severe, chronic cases show minimal improvement.
Which treatments are effective in reversing airway remodeling?
High-dose inhaled corticosteroids, targeted biologics (such as anti-IL5 and anti-IL4R agents), and bronchial thermoplasty (in some cases) have shown potential in reducing remodeling. Early diagnosis and consistent treatment improve chances of reversal.
Why is airway remodeling often permanent in severe asthma?
When remodeling progresses to extensive scar tissue formation, the changes become largely irreversible, limiting lung function despite treatment. In such cases, management focuses on preserving remaining airway function.
How can patients monitor airway remodeling progression?
Regular spirometry, fractional exhaled nitric oxide (FeNO) measurements, and periodic high-resolution CT scans help track airway structure and inflammation, guiding treatment adjustments to slow or reverse remodeling.