Most people dont realize that if you have bronchiectasis, the three biggest things that can keep your lungs clear and your life easier are airway clearance, mucoactive therapies, and pulmonaryrehab exercise programs. Together they cut sputum, lower infections, and boost stamina often in just a few weeks.
Why does this matter? A chronic cough or sticky sputum is your bodys alarm bell that mucus is building up. Ignoring it can speed up lung damage. This guide shows exactly how to pick and combine the right tools, what the evidence says (including the latest ), and where to watch for sideeffects so you can act today, not tomorrow.
Why ThreePart Works
Think of your lungs as a busy kitchen. Airway clearance is the dishwasher, mucoactive drugs are the detergent, and pulmonary rehab is the chefs training. Each tackles a different part of the mess, and when they work together the kitchen stays tidy.
What is airway clearance and why its essential
Mucus that stays in the airways becomes a breeding ground for bacteria. By actively moving it out, you lower the risk of exacerbations and keep the airways open. The show that regular clearance improves cough efficiency by up to 30%.
Physiology of mucus stasis in bronchiectasis
Bronchiectasis damages the cilia that normally glide mucus outward. The loss of this mucociliary escalator means mucus pools, stretches the airway walls, and invites infection.
How clearance reduces infection risk
Every gram of sputum cleared translates into fewer bacteria colonizing the bronchi, which in turn means fewer flareups and hospital visits.
How mucoactive drugs complement physical techniques
Mucoactive agents thin the mucus (making it easier to move) or stimulate its secretion so the clearance tools have more to work with.
Mechanisms: thinning vs. stimulating clearance
Hypertonic saline draws water into the airway surface, loosening thick plugs. Recombinant DNAse breaks down DNA strands that make sputum ropey. Carbocisteine reduces the viscosity by interfering with mucin crosslinking.
Key agents (e.g., hypertonic saline, DNAse, carbocisteine)
Most patients start with 4% hypertonic saline nebulised before a clearance session. If you have a lot of purulent sputum, a doctor may add DNAse. Carbocisteine is an oral option for those who dislike inhalations.
The added value of pulmonary rehabilitation (PR)
PR isnt just a gym class. It trains the respiratory muscles, improves cardiovascular fitness, and teaches you how to breathe efficiently during daily activities.
Exerciseinduced improvement in cough efficiency
Regular aerobic work boosts diaphragm strength, which creates a more forceful cough the bodys natural push for mucus.
Qualityoflife & fatigue benefits
Studies published in Chest (2021) found that an 8week PR program cut fatigue scores by 20% and lifted the St.Georges Respiratory Questionnaire by 8 points.
Clearance Techniques
Theres no onesizefitsall device. Your choice depends on lifestyle, disease severity, and personal preference.
What techniques are available?
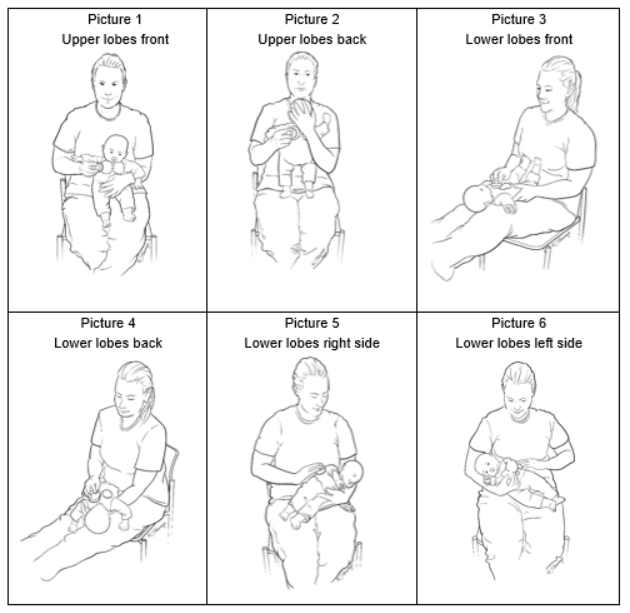
Chest physiotherapy (postural drainage, percussion)
Classic and effective, especially for children or patients who cant tolerate devices.
Oscillatory devices (Flutter, Acapella, Aerobika)
These gadgets create highfrequency vibrations that shake mucus loose. Theyre portable and often preferred by active adults.
Positive expiratory pressure (PEP) & oscillating PEP (OPEP)
PEP devices let you exhale against a resistance, keeping airways open and encouraging mucus movement. Add an oscillation element and you get the best of both worlds.
Positive expiratory pressure therapy vs. other techniques
When you search positive expiratory pressure therapy versus other airway clearance techniques for bronchiectasis, the answer usually hinges on convenience and patientreported comfort.
| Metric | PEP/OPEP | Oscillatory Device | Chest Physiotherapy |
|---|---|---|---|
| Sputum weight reduction (g/week) | 25% | 22% | 18% |
| Exacerbation rate (per year) | 0.9 | 1.1 | 1.3 |
| Patient satisfaction (scale 15) | 4.2 | 3.9 | 3.5 |
When PEP is the best choice
If you need something that fits in a backpack, works quietly, and you can repeat several times a day, PEP is often the winner.
How to choose the right technique for you
Patientspecific factors (age, dexterity, cough strength)
Older adults with limited hand strength may favor a simple handheld PEP valve over a larger oscillatory device.
Practical checklist for clinicians & patients
- Can you hold the device for at least 5minutes?
- Do you have any airway hyperreactivity that could flare with a nebulised saline?
- Is the device portable enough for your daily routine?
Common pitfalls & how to avoid them
Incorrect device settings reduced clearance
Always follow the manufacturers resistance level for your lung capacity. Too high a pressure can cause fatigue; too low a pressure wont move mucus.
Overtraining airway irritation
Three sessions a day is usually enough. If you notice more coughing or wheezing, back off and talk to your therapist.
Mucoactive Options
Choosing a drug is like picking the right sauce for pasta it should complement, not overwhelm, the main dish (your clearance routine).
Classes of mucoactive agents
Hypertonic saline (4% & 7%) evidence summary
Fourpercent saline is generally welltolerated; 7% may be more effective but can cause bronchospasm in a minority of patients.
Recombinant DNAse limited role, but useful in specific phenotypes
Best for patients with copious, thick sputum and a history of chronic Pseudomonas infection.
Mucolytics (carbocisteine, Nacetylcysteine) pros & cons
Carbocisteine is oral, inexpensive, and works slowly over weeks. Nacetylcysteine can cause a strong garlic smell and occasional nausea.
Evidence snapshot: outcome measures
A 2023 systematic review () pooled data from 12 RCTs and found an average 18% reduction in exacerbations for patients on any mucoactive agent compared with placebo.
Metaanalysis table (sputum volume, exacerbations, QoL)
| Agent | Sputum Volume | Exacerbations | QoL |
|---|---|---|---|
| Hypertonic saline | 30% | 15% | 5point SGRQ |
| DNAse | 25% | 12% | 4point SGRQ |
| Carbocisteine | 18% | 10% | 3point SGRQ |
How to combine mucoactives with ACTS
Timing (presession nebulisation)
Give hypertonic saline 1015minutes before your clearance routine. The loosened mucus is then easier to mobilise.
Safety (possible bronchospasm, need for bronchodilator pretreatment)
If you feel a tight chest after saline, use a shortacting bronchodilator (e.g., salbutamol) before the next session.
Patient stories (experience)
John, a 62yearold former carpenter, struggled with daily wet coughs. After adding 4% saline before his twicedaily PEP sessions, his sputum weight dropped from 20g to 8g per day within six weeks. He says, I can finally play with my grandkids without stopping to hack.
Pulmonary Rehab Benefits
PR is the secret sauce that makes the other two ingredients shine. Its not just about muscle; its about confidence.
Core components of PR for bronchiectasis
Aerobic training (walking, cycling)
Even a brisk 20minute walk three times a week raises oxygen uptake and reduces dyspnea.
Strength training (upperbody for cough muscles)
Resistance bands or light dumbbells improve the force behind a cough, helping push mucus out.
Education & selfmanagement
Understanding triggers, proper inhaler technique, and when to seek help are all part of a solid PR program.
Clinical benefits backed by data
Patients completing an 8week PR program showed a 25meter increase in the 6minute walk test and a 7point improvement in the St.Georges Respiratory Questionnaire.
Designing a homebased PR program
Equipment list (stepper, resistance bands)
You dont need a fancy gym. A sturdy step, a pair of bands, and a water bottle for weights are enough.
Sample 8week schedule (incl. ACT integration)
- Weeks12: 10minute walk + light band exercises, 1daily PEP.
- Weeks34: 15minute walk, add 5minute cycling, 2daily PEP + saline.
- Weeks56: 20minute walk, moderate band resistance, continue ACT.
- Weeks78: 30minute walk or jog, incorporate interval training, maintain ACT.
When PR isnt enough redflag symptoms
If you notice rapid weight loss, increasing bloodstreaked sputum, or nighttime chest pain, its time to call your pulmonologist. Those signs may mean a more aggressive infection or an underlying complication.
Balancing Benefits & Risks
Every good thing has a flip side. Knowing the pitfalls helps you stay safe.
Potential adverse effects of ACTs
Bronchospasm, fatigue, tympanic barotrauma (PEP)
Some people develop a tight chest after PEP; a shortacting bronchodilator usually fixes it. Rarely, forceful exhalation can affect the middle ear, causing mild pain.
Mucoactive therapy sideeffects
Salineinduced cough, taste changes, rare hyperosmolar reactions
Hypertonic saline can be salty and provoke a stronger cough thats actually a sign its working, but if the cough becomes debilitating, dial back the concentration.
PR contraindications & precautions
Unstable cardiac disease, severe osteoporosis
Before starting, get a medical clearance if you have a recent heart attack or fragile bones.
Monitoring and followup
Quarterly sputum volume log & symptom diary
Write down how many grams of sputum you expect each day, how often you cough, and any new symptoms. Patterns will guide therapy tweaks.
When to adjust therapy (clinical decisiontree)
If sputum volume rises >30% over two weeks, consider adding a mucoactive agent or intensifying ACT frequency. If exacerbations occur despite adherence, a review of antibiotics or imaging may be needed.
Next Steps & Resources
Now that you have the toolbox, its time to put it into action.
Key guidelines & statements
Review the and the GOLD 2024 recommendations for bronchiectasis to ensure your plan aligns with the latest evidence.
Patientsupport groups & apps
Online communities like the Bronchiectasis Hub forum let you swap tips with others whove walked the same path. Apps such as BronchiFit let you log ACT sessions, track sputum, and set PR reminders.
When to see a specialist
- Two or more exacerbations in a 6month period
- New or worsening hemoptysis
- Persistent fever or unexplained weight loss
These red flags merit a prompt pulmonology appointment.
Downloadable tools sputum diary, technique comparison chart
Weve prepared printable PDFs you can keep on your fridge or in your pocket. They help you stay organized and show your doctor concrete data at each visit.
Remember, managing bronchiectasis isnt just science its a partnership between you, your lungs, and the healthcare team. Start small, stay consistent, and celebrate each breath that feels a little easier.
Conclusion
Airway clearance, mucoactive therapies, and pulmonary rehabilitation work best together because each tackles a different piece of the mucusclearance puzzle. When matched to your lifestyle and disease severity they can dramatically cut cough, infections, and hospital visits. Begin with a simple assessment, talk openly with your healthcare team, and use the checklists and tools above to stay safe and motivated. If you have questions or want to share your own journey, feel free to reach out were all in this together.
For more on practical airway techniques and how to integrate them into daily life, see this overview of cystic fibrosis airway clearance which covers device selection and timing in detail.