In the next few minutes, well walk through why low sugar shows up during sepsis, what it means for patients of all ages (including newborns), and the most reliable ways to spot and treat it. Think of this as a friendly chat over coffeeno jargon, just clear, practical info you can trust.
Why Low Sugar Matters
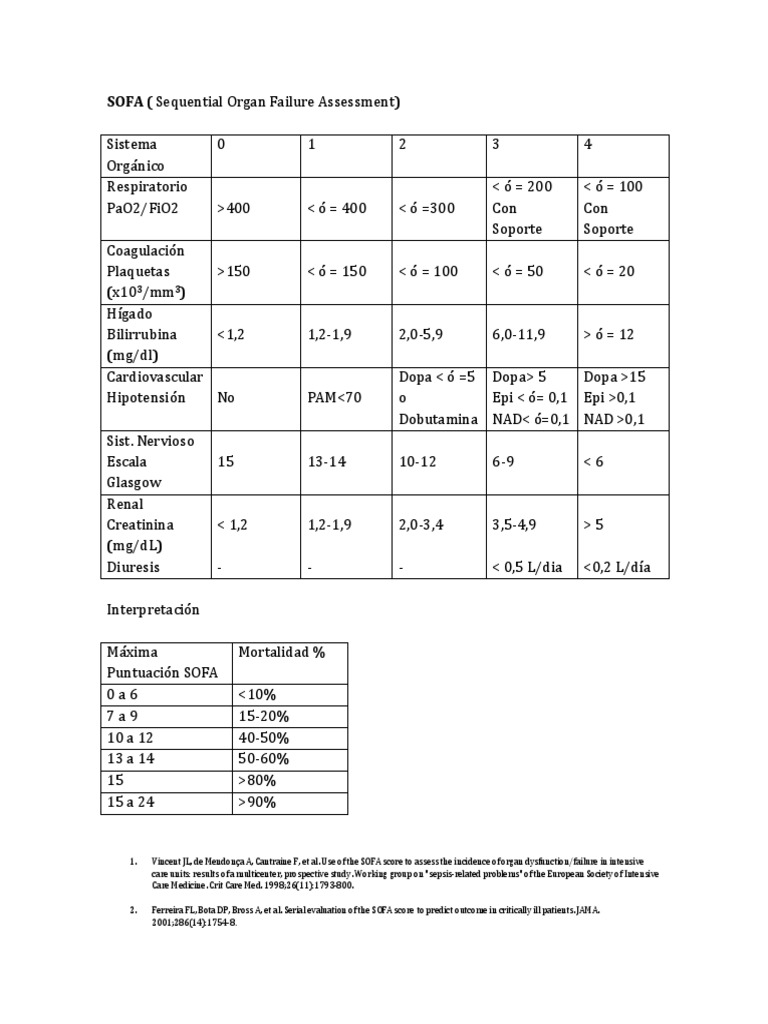
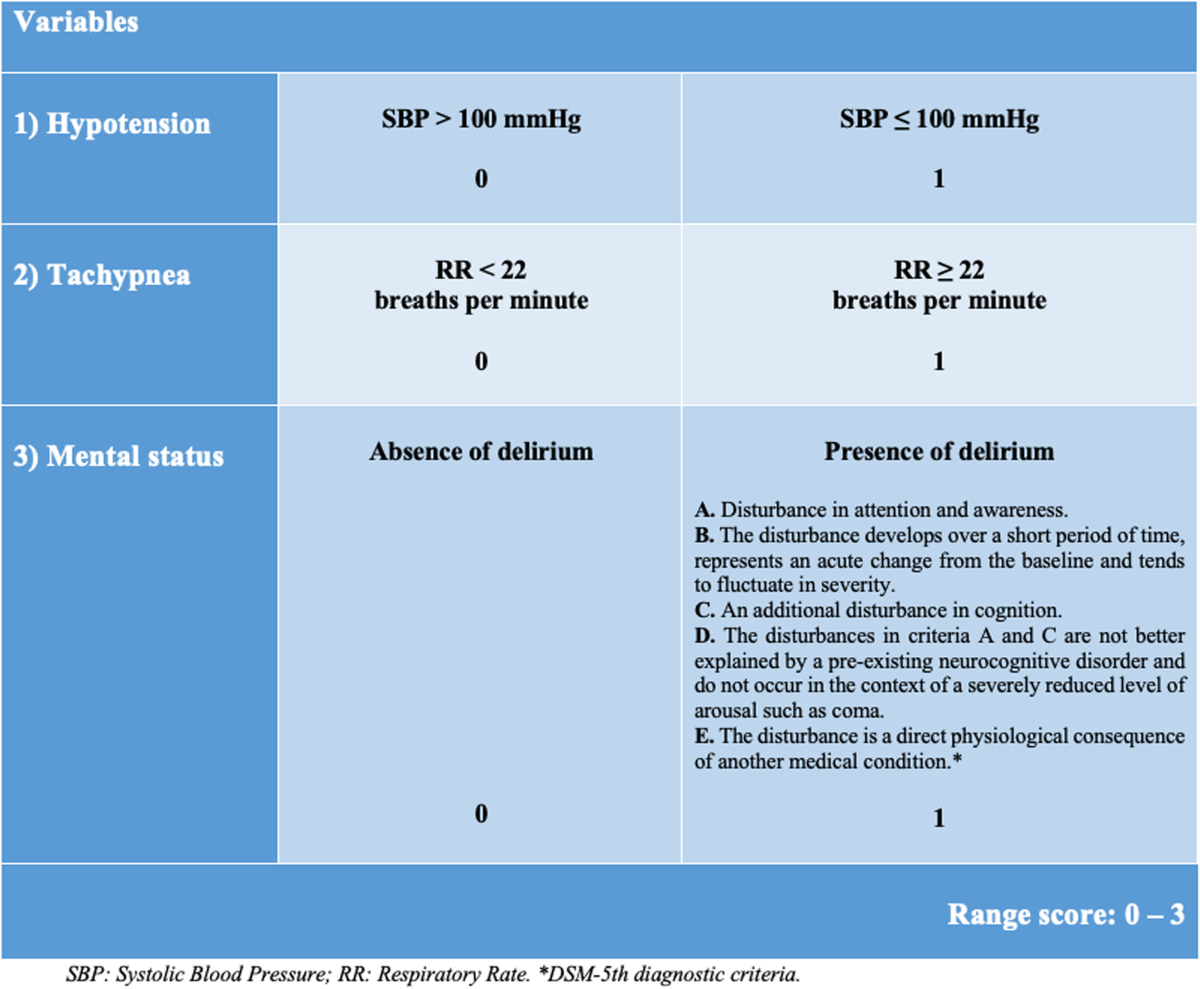
When you hear sepsis, the first thing that pops into most minds is a fever, rapid breathing, or a skyrocketing blood sugar level. Yet, for a surprising 1015% of patients admitted with severe infection, the blood glucose actually falls below 70mg/dL. That drop, known as hypoglycemia, is linked to a higher risk of organ failure and even death. For clinicians assessing severity, using validated tools such as the sepsis severity assessments can help identify patients at higher risk when hypoglycemia is present.
Why does it matter? Because the brain runs on glucose. When levels plunge, you can see confusion, shaking, or loss of consciousnesssymptoms that can mimic or mask the classic signs of sepsis. If we miss that lowsugar cue, we might delay a lifesaving intervention.
Sepsis Triggers Low Sugar
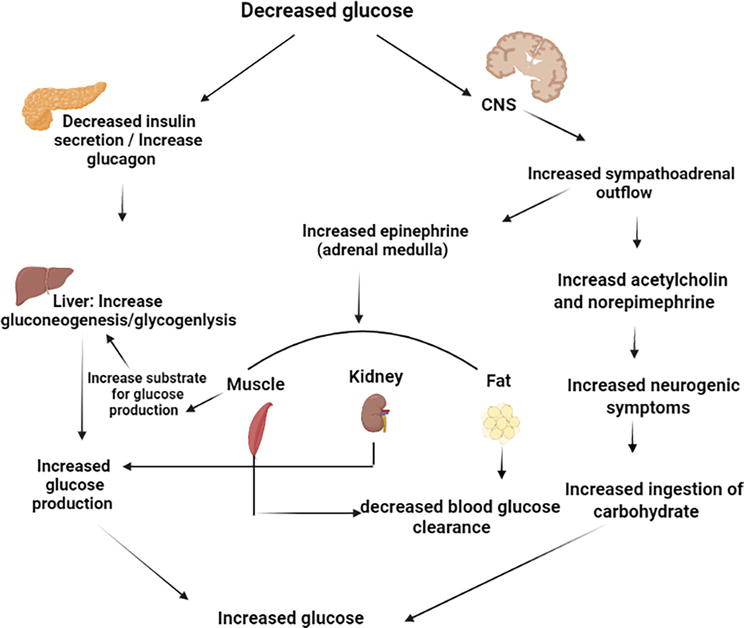
Sepsis throws the bodys metabolism into overdrive. Heres how it can steal your sugar:
- Metabolic overload: Cytokinesthose inflammatory messengersspeed up glycolysis, so cells gobble up glucose faster than the liver can replenish it.
- Impaired liver function: The livers ability to break down glycogen (the stored form of glucose) gets compromised, meaning the backup supply runs dry.
- Hormonal mismatch: Sepsis can blunt the stress hormones (cortisol, epinephrine) that normally keep blood sugar steady, especially in patients with adrenal insufficiency.
These mechanisms often act together, creating a perfect storm of low blood sugar at a time when your body is already struggling to maintain blood pressure, oxygenation, and organ perfusion.
What It Means for Patients
Studies have consistently shown that patients arriving with hypoglycemia in sepsis have a higher odds ratio for 30day mortality compared with those who are euglycemic or even hyperglycemic. A systematic review in reported mortality rates of about 45% for hypoglycemic patients versus 30% for those with normal glucose.
But it isnt all bleak. Recognizing the trend early and treating it promptly can swing the odds back in your favor. Thats why understanding both the risk and the remedy is essential.
Spotting the Problem
In the hustle of an ICU, its easy to focus on blood pressure, oxygen, and infection markers. Yet, a simple bedside glucose check can be a gamechanger. Heres a quick screening routine you can adopt:
- Check a fingerstick glucose on admission for any patient with suspected sepsis.
- Repeat every 46hours for the first 48hours, or sooner if mental status changes.
- Watch for classic hypoglycemia cues: sweating, tremor, irritability, or a foggy feeling.
When you notice a reading under 70mg/dL, treat it as an emergencyjust like you would for a sudden drop in blood pressure.
Treating the Drop
Now that youve caught the low sugar, lets talk about fixing it without causing a rebound high.
Acute Correction
Give a 50mL bolus of 50% dextrose (D50) intravenously over 12minutes. Recheck the glucose after 10minutes; if its still below 70mg/dL, repeat the bolus.
Target Range
Guidelines now recommend aiming for a glucose window of 140180mg/dL during the acute phase of sepsis. This range balances the risk of hypoglycemia with the dangers of hyperglycemia (which, by the way, is also common in sepsis and linked to its own set of complications).
Continuous Monitoring
After the initial correction, set up a sliding scale insulin drip if the glucose climbs above 180mg/dL. Adjust the rate gradually, watching for swings that could push you back into hypoglycemia.
Special Populations
Neonatal sepsis: Newborns have limited glycogen stores, so a 2mL/kg bolus of 10% dextrose is the first step, followed by a continuous infusion of 510mg/kg/min.
Diabetics: Infections can both increase insulin sensitivity and trigger stressinduced glucose release. If a diabetic patient on insulin develops sepsis, pause the routine insulin dose and adjust based on realtime glucose readings.
Balancing Risks
Its tempting to think lower is better when it comes to blood sugar, but tight control (80110mg/dL) has been shown to increase the risk of further hypoglycemic events, which can cause cardiac arrhythmias and brain injury. Modern sepsis protocols therefore favor a moderate targetenough to fuel the brain and muscles, but not so high that it fuels inflammation.
Ask yourself: Am I treating the number or the patient? The answer should always be the patient. Consider age, comorbidities, and the severity of the septic shock when deciding how aggressively to manage glucose. Using structured tools like the organ failure assessment approaches can help guide those decisions by clarifying which organs are most at risk when hypoglycemia occurs.
RealWorld Insights
In my own ICU experience, I recall a 68yearold man with pneumoniainduced septic shock. His glucose on admission was 52mg/dL. We gave D50, lifted his sugar to 110mg/dL, and then kept it steady around 150mg/dL with a lowdose insulin infusion. By day three, his blood cultures cleared, and he was walking out of the ICU with a smile.
Contrast that with a newborn who arrived with sepsis and a glucose of 38mg/dL. A rapid push of 10% dextrose and a continuous infusion kept his numbers stable, and he was discharged home two weeks later. These stories underline that early recognition and tailored treatment can turn a scary number into a survivable story.
Bottom Line
Seeing a low blood sugar reading in a patient with sepsis isnt a flukeits a red flag that the bodys metabolism is under severe stress. By understanding how sepsis causes hypoglycemia, staying vigilant with regular glucose checks, and applying balanced treatment strategies, we can dramatically improve outcomes.
If you or a loved one are navigating sepsis, remember: ask the care team about glucose monitoring right away. And if youve faced hypoglycemia during an infection, share your experience belowyour story might help someone else catch the warning sign early.
Stay curious, stay informed, and keep looking out for those quiet signals your body sends. Together we can turn knowledge into action, and action into recovery.
FAQs
What causes hypoglycemia in patients with sepsis?
Sepsis triggers a surge of inflammatory cytokines that accelerate glycolysis, deplete liver glycogen stores, and blunt stress‑hormone responses, all of which can drive blood glucose below normal levels.
How common is low blood sugar during severe infection?
Studies show that about 10‑15 % of patients admitted with severe sepsis develop hypoglycemia (glucose < 70 mg/dL), and this subgroup has a higher risk of organ failure and mortality.
What are the immediate steps to treat hypoglycemia in sepsis?
Administer a 50 mL intravenous bolus of 50 % dextrose (D50) over 1‑2 minutes, re‑check glucose after 10 minutes, and repeat if needed. Follow with a glucose infusion to keep levels in the target range.
What glucose target should be maintained in septic patients?
Current guidelines recommend keeping blood glucose between 140 – 180 mg/dL during the acute phase of sepsis to avoid both hypoglycemia and hyperglycemia‑related complications.
Are there special considerations for newborns or diabetic patients?
Newborns receive a 2 mL/kg bolus of 10 % dextrose followed by a 5‑10 mg/kg/min infusion. Diabetic patients should have routine insulin paused and dosing adjusted based on real‑time glucose readings.