If you or someone you love is battling acute myeloid leukemia (AML), the idea that the disease could reach the brain feels like a nightmare you don't want to imagine. Here's a straightforward, nofluff guide that tells you how often CNS AML occurs, what symptoms to watch for, how doctors diagnose it, and what treatment paths are available today.
How Common Is CNS AML
What does the latest data say about incidence?
While AML itself is a fairly common blood cancer, involvement of the central nervous system (CNS) is relatively rare. Reports from clinical reviews and other peerreviewed sources estimate that only about 11.5% of patients have CNS disease at the time of initial diagnosis. The number climbs to roughly 24% during relapse, especially in cases that are refractory to standard chemotherapy.
Why is it more frequent in relapsed or refractory AML?
When leukemia returns, there's often a higher overall disease burden and the protective bloodbrain barrier can become compromised. Certain AML subtypesparticularly those with monocytic featurestend to infiltrate the meninges more easily, and prior intense chemotherapy can weaken the barrier, letting blasts slip into the cerebrospinal fluid (CSF).
Key Statistics (20202025)
| Study | Patients | CNSAML at Diagnosis | CNSAML at Relapse | Total % |
|---|---|---|---|---|
| UpToDate (2025) | 11.5% | 24% | <5% | |
| Blood Advances 2023 | 2,045 | 1.1% | 1.8% (postallo HSCT) | |
| NCBI PMC 2023 | 1,200 | 1.2% |
Signs and Symptoms
What are the all CNS involvement symptoms patients report?
The nervous system doesn't whisper; it shouts when it's being invaded. Common complaints include:
- Persistent or worsening headache
- Newonset seizures or focal neurological deficits (like weakness on one side)
- Cranial nerve palsies for example, double vision or facial droop
- Changes in mental status confusion, sluggishness, or sudden personality shifts
- Visual disturbances or hearing loss
If any of these show up while you're undergoing AML treatment, it's worth raising the alarm right away.
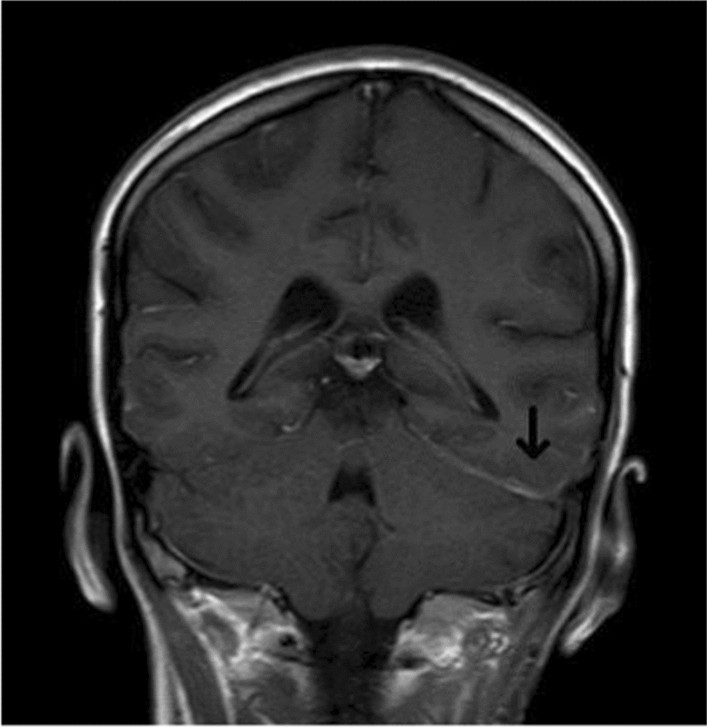
How is AMLbrain spread detected on imaging?
Magnetic resonance imaging (MRI) with gadolinium contrast is the gold standard. Radiologists look for leptomeningeal enhancement (a thin, glowing lining around the brain) or small parenchymal nodules that light up on T1weighted images. Occasionally, diffusionweighted imaging (DWI) reveals restricted diffusion, a sign of dense blast infiltration.
Radiology Checklist for AMLBrain Involvement
- Diffuse leptomeningeal enhancement
- Intraparenchymal nodules or masslike lesions
- Ependymal involvement of the ventricles
- Restricted diffusion on DWI sequences
Diagnosing CNS AML
When should a lumbar puncture (LP) be performed?
Guidelines suggest an LP at diagnosis for highrisk patientsthose with monocytic AML, a whitebloodcell count above 10010^9/L, or any neurologic symptoms. Even if you feel fine, a prophylactic LP can catch hidden disease before it becomes symptomatic.
What does CSF analysis reveal?
A CSF blast count of 5% or the presence of abnormal immunophenotype on flow cytometry confirms CNS involvement. Cytochemistry (myeloperoxidase staining) can help differentiate blasts from reactive cells, while molecular testing (e.g., FLT3ITD) may guide targeted therapy.
Expert Tip Avoiding FalseNegatives
To maximize yield, collect at least 10 mL of CSF, process the sample within 30 minutes, and run both morphology and flow cytometry. Delays or small volumes can let fragile blasts disappear, giving a falsenegative result.
Prognosis Overview
Is prognosis worse with CNS involvement?
Unfortunately, yes. Studies indicate overall survival drops by roughly 1530% compared to AML without CNS disease. A retrospective analysis published in a hematology review showed a median overall survival of 12 months for patients with CNS AML at diagnosis versus 22 months for those without.
Does early detection improve outcomes?
Early detection definitely helps. Patients who receive intrathecal therapy promptly after a positive LP tend to achieve longer remission durations. One analysis reported a median remission of 9 months for earlytreated patients versus 5 months for those whose CNS disease was discovered later.
Comparative Outcomes
| Group | 2Year OS | Median OS (months) | Relapse Rate |
|---|---|---|---|
| AML + CNS (diagnosis) | 35% | 12 | 65% |
| AML + CNS (relapse) | 28% | 9 | 72% |
| AML no CNS | 55% | 22 | 40% |
Treatment Strategies
What is CNS AML prophylaxis and who gets it?
Prophylaxis means preventing CNS disease before it starts. Highrisk patients receive intrathecal (IT) methotrexate (MTX) and cytarabine (AraC) during induction chemotherapy. The goal is to saturate the CSF with drug levels that would kill any lurking blasts.
How are isolated CNS relapse AML cases managed?
When the CNS is the sole site of relapse, treatment intensifies:
- Repeated intrathecal MTX and AraC (usually 34 doses per week)
- Systemic highdose cytarabine (23 g/m2) to reach the CSF via the bloodstream
- Consider cranial irradiation (typically ~12 Gy) if blasts persist after chemotherapy
This combination aims to eradicate disease from both sides of the bloodbrain barrier.
StepbyStep Treatment Algorithm
- Induction Standard 7+3 regimen (cytarabine + anthracycline) plus IT MTX/AraC.
- Reassessment CSF analysis on Day 14 to gauge response.
- Consolidation Highdose cytarabine plus a second round of IT chemotherapy.
- Maintenance/HSCT For eligible patients, an allogeneic stemcell transplant after achieving CNS remission.
What are the risks and sideeffects of intrathecal therapy?
IT drugs can irritate the lining of the brain and spinal cord, leading to chemical meningitis (fever, neck stiffness) or, rarely, neurotoxicity such as peripheral neuropathy. Prehydration, a short course of steroids, and meticulous technique dramatically lower these risks.
Patient Story Snapshot
Jane, a 42yearold mother, was diagnosed with monocytic AML. Two months into induction, she developed a persistent headache and mild confusion. A quick LP revealed 12% blasts. Her team launched intensive IT MTX plus highdose cytarabine, and within six weeks her CSF was clear. She went on to a successful transplant and is now celebrating her third remission anniversary. Jane's experience underscores how vigilance and rapid action can turn a scary situation into a hopeful turnaround.
FollowUp Care
How often should CSF be rechecked after treatment?
Most hematology centers repeat a lumbar puncture at the end of induction, after each consolidation block, and then every 36 months for the first two years. Frequent monitoring catches early reemergence before symptoms become severe.
When is CNS imaging indicated during remission?
If you develop new neurologic signsor if CSF studies turn up abnormal cellsan MRI with contrast is the next step. Routine imaging without symptoms isn't standard, but some highrisk protocols include a baseline MRI after completing IT therapy.
Checklist for Patients & Caregivers
- Maintain a symptom diary (headache intensity, visual changes, weakness)
- Schedule LP dates in your calendar; don't miss them
- Know emergency signs: sudden seizures, rapid mental decline, or new focal deficits
- Keep contact information for your hematology team handy
Bottom Line Balancing Benefits & Risks
CNS involvement in AML is uncommon, but when it happens it's serious. Early detection, timely intrathecal therapy, and coordinated systemic treatment give patients the best chance for prolonged remission, while careful followup helps limit neurotoxic sideeffects. The journey can feel overwhelming, but knowing what to look for and how it's treated equips you to act confidently.
Conclusion
We've covered how often CNS AML shows up, the warning signs that should set off alarms, how doctors confirm the diagnosis, and what treatment options existfrom prophylactic intrathecal methotrexate to aggressive management of isolated CNS relapse. Keeping a close eye on symptoms, staying on schedule with lumbar punctures, and maintaining open communication with your care team are key to navigating this complex part of AML care.
If this guide helped you feel a bit more in control, please share it with anyone you know who might be facing AML. Have questions or personal experiences you'd like to add? Drop a comment belowyour story could be the reassurance another reader needs. And if you'd like to stay updated on the latest leukemia research, consider signing up for our newsletter; we promise to keep it friendly, factual, and focused on what matters most to you.
For related information about treatment considerations during pregnancy, see AML pregnancy treatment, which covers risks and options when AML occurs during pregnancy.
FAQs
What is CNS AML?
CNS AML refers to acute myeloid leukemia that has spread to the central nervous system, affecting the brain or spinal cord.
How common is CNS involvement in AML?
CNS involvement is rare, occurring in about 1-1.5% of AML cases at diagnosis and up to 2-4% during relapse.
What are the symptoms of CNS AML?
Symptoms include headaches, seizures, confusion, weakness, vision changes, and sometimes no symptoms at all.
How is CNS AML diagnosed?
Diagnosis is made through lumbar puncture and CSF analysis, often supported by MRI imaging.
What treatments are available for CNS AML?
Treatment includes intrathecal chemotherapy, high-dose systemic chemotherapy, and sometimes cranial irradiation.