Looking for a quick answer on how an MRI helps stage cervical cancer? In a nutshell, MRI is the goldstandard tool that shows the size of the tumor, whether its reached nearby tissues, and if any lymph nodes are involved. Those details steer every treatment decision from surgery to radiation.
Getting a cancer diagnosis can feel like stepping into a storm. Im here to walk you through what an MRI actually does, what youll see on the scan, and how to talk about the results with your care team all in plain language, no medical jargon overload.
Why MRI Matters
What does cervical cancer MRI actually assess?
An MRI (Magnetic Resonance Imaging) provides a detailed, threedimensional picture of the cervix and surrounding structures. Unlike CT or ultrasound, it captures the softtissue contrast that reveals:
- The exact dimensions of the tumor (crucial for FIGO staging).
- Whether the tumor has invaded the parametrial tissue, the vaginal cuff, or the uterine body.
- The appearance of pelvic lymph nodes size, shape, and signal characteristics.
All of this information is compiled into the cervical cancer radiology staging report that your oncologist will use to tailor therapy. For patients also managing other cancers, resources on topics like prostate cancer outlook can be useful for broader treatment planning discussions.
How does MRI fit into the 2018 FIGO staging system?
The International Federation of Gynecology and Obstetrics (FIGO) updated its staging in 2018 to rely heavily on imaging. , MRI is the preferred modality for assessing parametrial invasion (stageIIB) and nodal disease (stageIIIC). Thats why most cancer centers request an MRI before finalizing a treatment plan.
Key advantages over ultrasound & CT
| Feature | Ultrasound | CT | MRI |
|---|---|---|---|
| Softtissue contrast | Poor | Moderate | Excellent |
| Radiation exposure | None | Yes | None |
| Parametrial assessment | Limited | Limited | Reliable |
| Lymphnode characterization | Very limited | Size only | Size + morphology |
In short, MRI gives you the clearest view without the ionising radiation that CT brings.
Standard MRI Protocol
Typical sequence checklist
When you walk into the scanner, the technologist will run a series of sequences designed to capture every angle of the cervix:
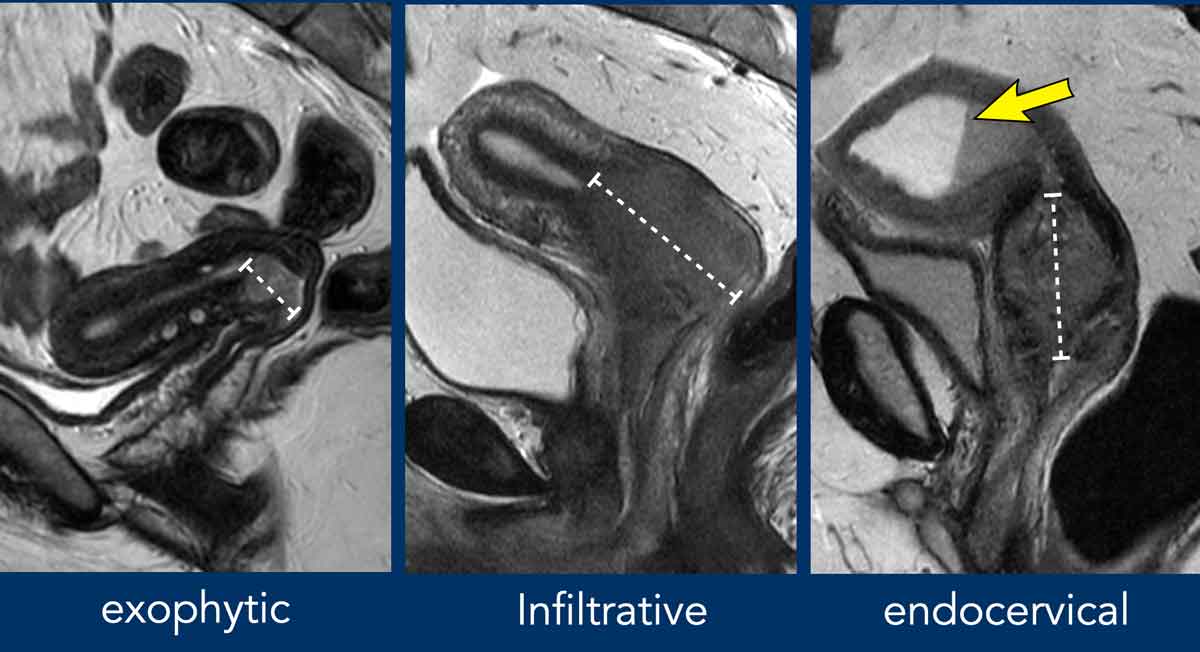
- T2weighted sagittal and axial shows anatomical detail and tumor margins.
- Diffusionweighted imaging (DWI) highlights cellular density; cancer usually appears bright.
- T1weighted with gadolinium contrast enhances vascular tumor tissue and helps differentiate scar from active disease.
- Highresolution T2weighted perpendicular to the cervical canal essential for measuring depth of stromal invasion.
All of these are part of the cervical cancer MRI protocol youll find on sites like Radiology Assistant, which many radiology departments follow.
Patient preparation tips
To get the best images youll want a partially full bladder (it lifts the uterus and reduces artefacts) and an empty bowel (so gas doesnt distort the view). Some centers give an antiperistaltic agent like hyoscine butylbromide to quiet the intestines. And, of course, let the technologist know if youre claustrophobic they can offer a mild sedative or an openMRI option.
How long does the exam take?
A complete cervical cancer MRI usually lasts 3045 minutes, including positioning and the brief breathholds required for certain sequences. If contrast is used, add another 510 minutes for the injection and postcontrast imaging.
Interpreting Staging Images
Reading tumor size on T2weighted images
The radiologist measures the greatest tumor diameter in three orthogonal planes. According to a systematic review in , a size >4cm typically pushes the disease into stageIIB if parametrial invasion is also seen.
Identifying parametrial invasion & vaginal extension
On T2, a tumor that crosses the lowsignal cervical stromal ring into the highsignal parametrial fat signals stageIIB. If the lesion extends into the upper third of the vagina, thats stageIIA. The radiology assistant at Radiopaedia illustrates these boundaries with colourcoded arrows a handy visual aid for any patient wanting to understand the report.
Assessing lymphnode involvement
Size alone isnt enough. Nodes >10mm, irregular borders, or a loss of the fatty hilum raise suspicion. DWI adds a highbvalue signal that further supports metastatic involvement. A 2023 AJR review notes that MRI with DWI improves nodal detection sensitivity from 60% (sizeonly) to about 85%.
When MRI shows no residual disease after therapy
Posttreatment MRI can demonstrate fibrosis (low signal on T2) versus active tumour (high signal on DWI). A lack of restricted diffusion plus a stable or shrinking mass usually means the cancer has responded well. Your radiologist will compare the current scan with baseline images to make that call.
Benefits and Risks
Clinical benefits
Accurate staging means you get the right treatment the first time sparing you from unnecessary surgery or overly aggressive radiation. Studies have shown that MRIguided planning reduces the rate of positive surgical margins by up to 30%.
Patientcentred benefits
Because MRI does not use ionising radiation, its safe for repeated followup scans. The detailed images also give patients a clearer picture of whats happening inside their bodies, which can lessen anxiety.
Potential risks
Most risks are mild:
- Contrast allergy rare, but inform your doctor if youve had reactions before.
- Claustrophobia many centres offer openMRI or mild sedation.
- Falsepositives sometimes scar tissue can look like tumour; a followup scan or biopsy can clarify.
- Pregnancy MRI without gadolinium is generally considered safe, but discuss any concerns with your obstetrician.
MRI vs Other Scans
Ultrasound: when its useful & where it falls short
Transvaginal ultrasound is great for initial assessment and guiding biopsies, but it cant reliably show parametrial invasion or nodal disease. It remains a firstline tool for women who cant undergo MRI.
CT: role in detecting distant metastases
CT scans cover the entire abdomen and chest, making them useful for spotting lung or liver spread. However, they lack the softtissue detail needed for local staging, which is why CT is usually paired with MRI rather than replacing it.
PETCT: complementary functional information
PETCT adds metabolic data, highlighting hyperactive cancer cells. Its particularly helpful when MRI findings are ambiguous or when you need to confirm distant disease. A 2022 metaanalysis found PETCT raised overall staging accuracy when combined with MRI.
Comparison matrix
| Modality | Accuracy (local) | Radiation | Cost | Availability |
|---|---|---|---|---|
| Ultrasound | Moderate | No | Low | High |
| CT | Fair | Yes | Moderate | High |
| PETCT | High (combined) | Yes | High | Moderate |
| MRI | Very high | No | High | Moderate |
Patient FAQ Guide
Do I need to fast before the scan?
Usually no, unless youre receiving contrast. In that case, a light meal 23 hours before the exam is fine.
Can I wear jewelry or metal?
All metal must be removed watches, necklaces, and even some piercings. The technologist will give you a locker for personal items.
How soon will I get results?
Radiology reports are typically available within 2448hours. Your oncologist will discuss the findings in a followup appointment.
What if I cant stay still?
Talk to the scanner staff. They can provide cushions, a mild sedative, or an openMRI system that feels less confining.
Discussing MRI Findings
Key terms to know
When your doctor talks about parametrial involvement, theyre referring to tumour spread beyond the cervix into the surrounding fatty tissue. Highsignal on DWI means the lesion is likely still active. Knowing these phrases helps you ask focused questions.
Preparing questions for your oncologist
Write down things like:
- What stage does the MRI suggest?
- Are there any suspicious lymph nodes?
- How will this stage affect my treatment options?
- Do you recommend a second opinion from a radiology specialist?
When to seek a second radiology opinion
If the report mentions probable invasion or borderline nodal size, a second read by a subspecialist in gynecologic oncology imaging can clarify. Many cancer centers have a cervical cancer radiology assistant service that offers this secondlook at no extra charge.
Conclusion
In essence, a cervical cancer MRI is the most precise way to map the tumor, decide the stage, and plan the right treatment. It offers excellent softtissue detail without radiation, and the standardized protocol means youll get consistent, reliable information each time. By understanding the benefits, the modest risks, and how to discuss the findings with your care team, you become an active participant in your own health journey.
If this guide helped clear up some of your questions, feel free to share it with anyone you know facing a cervicalcancer diagnosis. And remember, youre not alone lean on your doctors, ask the right questions, and keep the conversation going. Have more questions? Drop a comment below; were here to support each other.
FAQs
How does a cervical cancer MRI differ from an ultrasound?
Unlike ultrasound, MRI provides excellent soft‑tissue contrast, allowing clear visualization of parametrial invasion and lymph‑node characteristics without ionising radiation.
What sequences are included in a standard cervical cancer MRI?
The typical protocol uses T2‑weighted sagittal and axial images, high‑resolution T2 perpendicular to the cervical canal, diffusion‑weighted imaging (DWI), and T1‑weighted images after gadolinium contrast.
Can an MRI determine if the cancer has spread to lymph nodes?
Yes. MRI evaluates node size, shape, loss of fatty hilum and diffusion restriction, which together improve detection of metastatic lymph‑node involvement.
Is contrast always required for a cervical cancer MRI?
Gadolinium contrast is usually administered to highlight vascular tumor tissue and differentiate scar from active disease, but a non‑contrast study may be done if contraindicated.
How soon will I receive the MRI results?
Radiology reports are typically available within 24–48 hours, after which your oncologist will discuss the findings and staging with you.