If you ever find yourself in the scary situation where meningitis is suspected, the first thing doctors do is start empiric meningitis treatment right awayno waiting for lab results. In most cases the goto combo is a highdose cephalosporin (like ceftriaxone or cefotaxime) plus vancomycin, and sometimes ampicillin or acyclovir depending on age and risk factors.
Getting the right drugs fast can be the difference between a full recovery and serious complications. Below we'll walk through exactly what empiric means, which antibiotics are used for adults and kids, how long treatment usually lasts, and what you need to watch out for. Think of it as a friendly cheatsheet you can share with a loved one or keep handy in case the unexpected happens.
Why Empiric Matters
What empiric really means
In medicine, empiric means treating based on the most likely germs before any cultures tell us for sure. It's like guessing the flavor of a mystery smoothie based on the fruit you see on the tableoften you're right, and you've got to act fast.
The clock is ticking
Bacterial meningitis can progress from fever to severe neurologic injury in a matter of hours. Studies show mortality jumps dramatically after the first six hours without appropriate antibiotics. That urgency is why guidelines push for immediate empiric therapy.
Mortality data (CDC 2024)
According to a , early, appropriate antibiotics cut mortality by roughly 30%.
Goals of empiric therapy
- Rapid bacterial killing
- Penetration of the bloodbrain barrier
- Broad coverage of the most common pathogens
Adult Core Regimen
Standard firstline combo
The cornerstone for adults is:
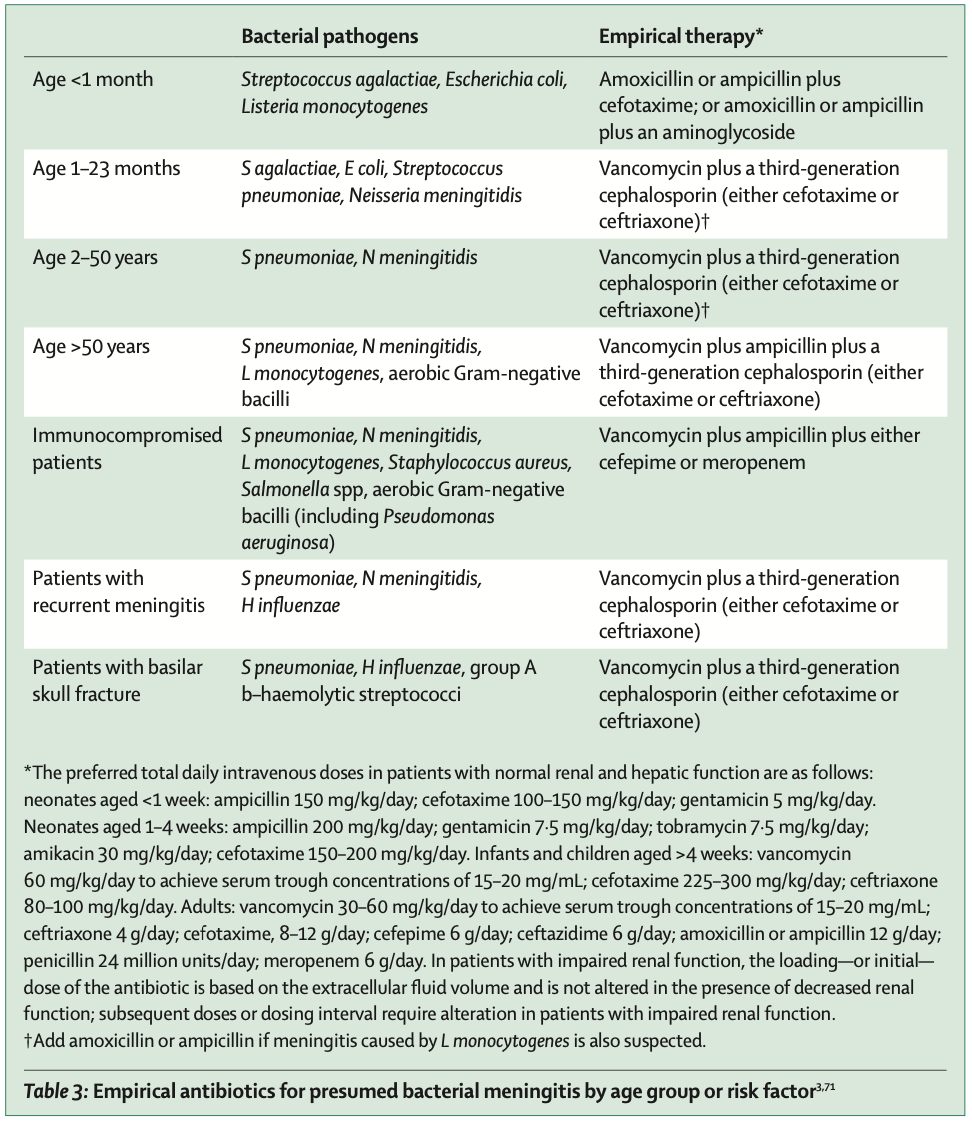
- Ceftriaxone 2g IV every 12hours or Cefotaxime 2g IV every 46hours
- Vancomycin 1520mg/kg IV every 812hours (adjusted for MIC)
- Ampicillin 2g IV every 4hours if Listeria risk (age >50, immunocompromised, pregnancy)
When acyclovir joins the party
If HSV1 encephalitis or viral meningitis is on the differential, add acyclovir 10mg/kg IV every 8hours. It's safe to start both antibiotics and antivirals until the PCR results come back.
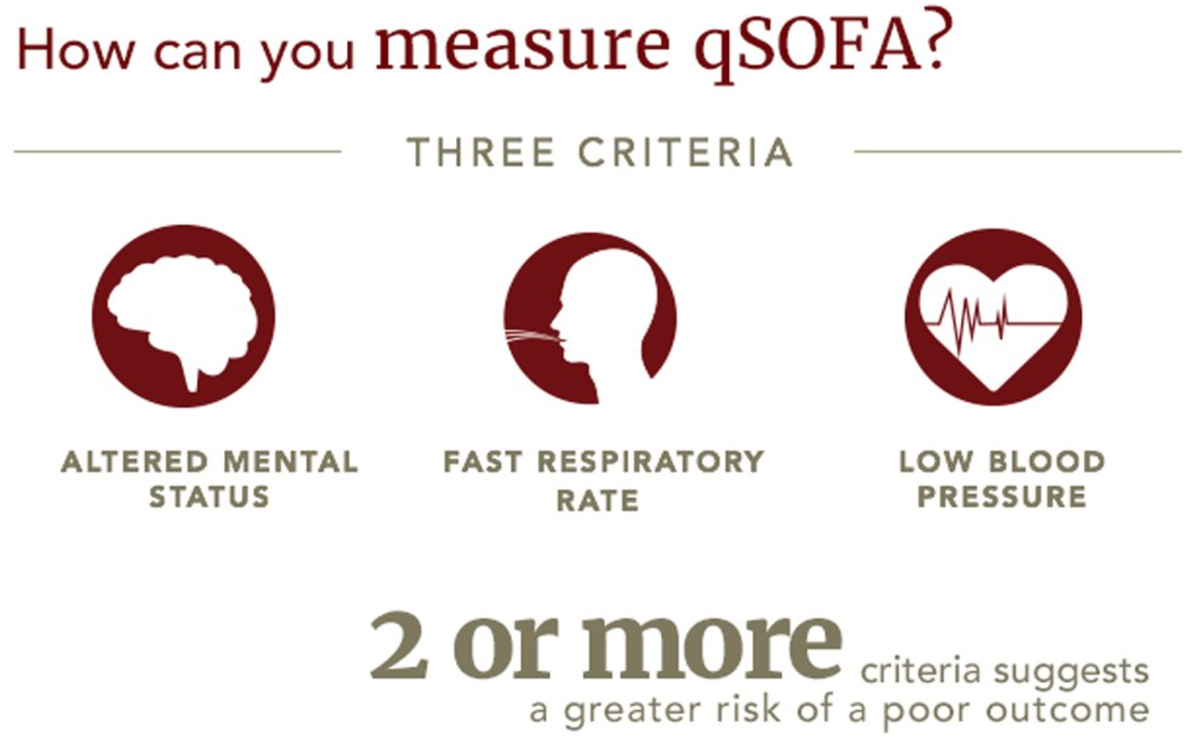
When clinicians worry about overall organ dysfunction from severe infection, they may also use scores such as the SOFA score to track organ failure and guide escalation of care.
Typical treatment length
How long do we keep the drugs going? In general:
- Pneumococcal meningitis: 1014days
- Neisseria meningitidis: 710days (often 10days for safety)
- Listeria: 1421days
- If viral, acyclovir usually runs 1421days
Adult duration table
| Presumed Pathogen | Recommended Duration |
|---|---|
| Pneumococcus | 1014 days |
| Neisseria meningitidis | 710 days |
| Listeria monocytogenes | 1421 days |
| HSV1 (viral) | 1421 days of acyclovir |
Pediatric Empiric Care
Agespecific bugs
Kids aren't just small adults; the microbes that love a toddler's brain differ from those that target a teenager. Common culprits include Group B Streptococcus, Haemophilus influenzae, Neisseria meningitidis, and Listeria in newborns.
Recommended pediatric regimen
- Cefotaxime 50mg/kg IV every 6hours or Ceftriaxone 100mg/kg IV every 12hours
- Vancomycin 1520mg/kg IV every 8hours (if penicillinresistant Streptococcus is a concern)
- Ampicillin 50mg/kg IV every 6hours for neonates or when Listeria risk exists
Acyclovir for children
Just like in adults, acyclovir is added when HSV1 is on the radar. Dosing is 20mg/kg IV every 8hours for infants, tapering to 10mg/kg for older kids.
Case vignette
Sixmonthold Emma arrived with fever, a bulging fontanelle, and a stiff neck. The ER started cefotaxime, vancomycin, and ampicillin immediately. CSF culture later revealed Group B Streptococcus, so the team stopped vancomycin after 48hours and completed a 14day cefotaxime course. Emma recovered fully with no neurologic sequelae.
Guideline Influence
Key sources
All the recommendations above come from the latest guideline updates, CDC clinical recommendations, and WHO consensus documents. These bodies update their meningitis treatment guidelines every few years to reflect emerging resistance patterns.
Quicklook checklist
Print the downloadable PDF checklist (linked on the CDC page) and keep it in your emergency kit. It reminds you of drug choices, doses, and when to add ampicillin or acyclovir.
Balancing Benefits & Risks
Why early therapy saves lives
Starting empiric antibiotics within the first hour of suspicion reduces mortality by up to one third and improves neurologic outcomes. The earlier, the better mantra isn't just a sloganit's backed by hard data.
Common side effects you should know
- Cephalosporins: rash, mild diarrhea, occasional gallbladder sludge
- Vancomycin: nephrotoxicity, ototoxicity at high trough levels
- Acyclovir: renal impairment, rare neurotoxicity (confusion, tremor)
Monitoring checklist
Before and during treatment, keep an eye on:
- Serum creatinine and urine output (for vancomycin/acyclovir)
- Drug trough levels for vancomycin
- Allergy history (especially penicillin or cephalosporin allergies)
Resistance concerns
Even in emergencies, we don't want to fuel antimicrobial resistance. That's why deescalation (switching to a narrowerspectrum drug once cultures return) is a critical step, and why stewardship programs monitor empiric choices closely.
Patient Practical Steps
What to expect in the ER
When you walk into the emergency department with a suspected meningitis case, the team will:
- Draw blood and a lumbar puncture as fast as safely possible.
- Start the empiric antibiotic cocktail within minutes.
- Monitor vitals, give steroids if indicated (dexamethasone for pneumococcal meningitis), and assess for complications.
Questions you can ask your doctor
Being an active participant helps you feel more in control. Consider asking:
- Which bugs are we covering with the current regimen?
- When will we know the exact pathogen?
- Do we need steroids, and why?
- How long will I be on IV antibiotics?
Home care after discharge
Once you're stable enough to leave the hospital, you may switch from IV to oral antibiotics (if the pathogen allows). Continue the full course, keep followup labs, and watch for any new headaches, fever, or rash.
Case Studies (Experience Highlights)
Adult emergency success
John, 62, arrived with fever and confusion. The ER gave ceftriaxone, vancomycin, and ampicillin right away. CSF culture grew Listeria monocytogenes. Because ampicillin was already on board, his doctors continued it for 21days, and he made a full recovery.
Pediatric triumph
Sara, a newborn, presented with poor feeding and a bulging fontanelle. Empiric treatment began with cefotaxime and ampicillin. Blood cultures later identified Group B Streptococcus. The team stopped ampicillin after 48hours and completed a 14day cefotaxime course. Sara is now thriving.
Future Outlook
New drugs on the horizon
Researchers are testing cefiderocol, a siderophorelinked cephalosporin that can breach resistant Gramnegative walls. Early trials look promising for cases where standard drugs fail.
Rapid diagnostics changing empiric
Pointofcare PCR panels can identify bacterial DNA within an hour, potentially shrinking the window of broadspectrum empiric therapy. In the future, you might receive a targeted antibiotic in under 60minutes instead of the current covereverything approach.
Conclusion
When meningitis looms, swift empiric meningitis treatment is the lifesaverthink highdose ceftriaxone or cefotaxime plus vancomycin, with ampicillin added for Listeria risk and acyclovir when viruses are a concern. Adults and children follow similar principles but differ in dosing and the bugs they face. Stick to the recommended empiric treatment for meningitis in adults or pediatrics, watch for side effects, and deescalate once cultures guide you. Keep the latest meningitis treatment guidelines handy, ask your care team questions, and remember that early action, informed choices, and good followup are the keys to a full recovery.
FAQs
What is empiric meningitis treatment?
Empiric meningitis treatment is the immediate initiation of broad-spectrum antibiotics targeting the most likely pathogens before specific lab results are available, to prevent rapid disease progression and reduce mortality.
Which antibiotics are commonly used for empiric meningitis treatment in adults?
The typical first-line regimen includes ceftriaxone or cefotaxime plus vancomycin. Ampicillin is added if there is risk for Listeria, such as in adults over 50, immunocompromised, or pregnant patients.
How long does empiric meningitis treatment usually last?
Treatment duration varies by pathogen: 10-14 days for pneumococcus, 7-10 days for Neisseria meningitidis, and 14-21 days for Listeria and viral meningitis with acyclovir.
When is acyclovir added to empiric meningitis treatment?
Acyclovir is added when herpes simplex virus (HSV) encephalitis or viral meningitis is suspected, dosing adults at 10 mg/kg IV every 8 hours until viral PCR results clarify the diagnosis.
What are the main risks or side effects of empiric meningitis antibiotics?
Common side effects include rash and diarrhea from cephalosporins, kidney and ear toxicity from vancomycin at high levels, and possible renal impairment or rare neurotoxicity from acyclovir.