Understanding Central Sleep Apnea
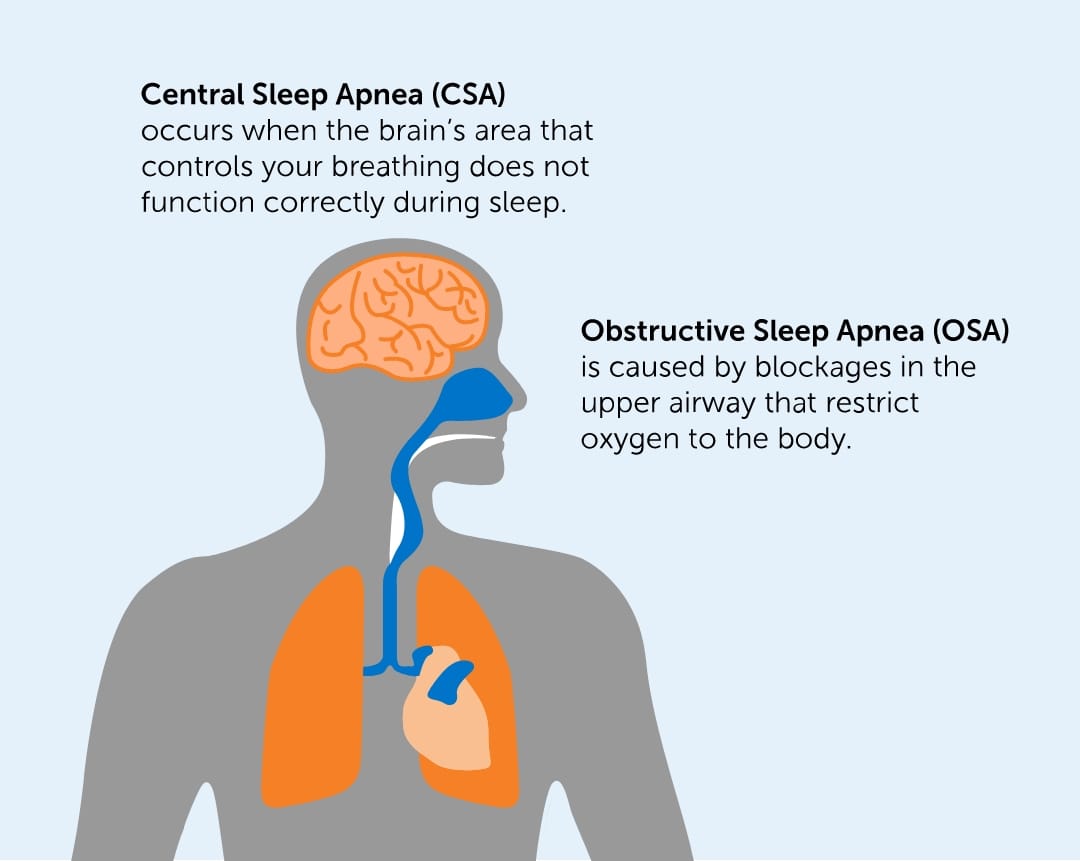
First things first: CSA isnt the same as the more common obstructive sleep apnea (OSA). In CSA, the brains breathing center simply forgets to send the go signal to the diaphragm. Imagine a conductor who forgets to cue the orchestrasilence follows until the cue comes back.
What is CSA?
Think of your brain as a tiny airtraffic controller. It monitors carbon dioxide (CO) levels and, when they rise, tells the diaphragm to take a breath. When that message gets lost, you experience a brief pauseusually just a few secondsbut it can happen dozens of times a night.
CSA vs. Obstructive Sleep Apnea
| Feature | Central Sleep Apnea | Obstructive Sleep Apnea |
|---|---|---|
| Root cause | Brain fails to send breathing signal | Physical blockage of airway |
| Typical breathing pattern | Flat line of airflow (no effort) | Effort continues, but airflow stops |
| Common treatments | Address underlying condition, ASV, oxygen | CPAP, weight loss, surgery |
Primary Medical Causes
When we talk about the big hitters that trigger CSA, they usually fall into three families: neurological, cardiac, and metabolic/systemic.
Neurological Causes of Central Sleep Apnea
Anything that messes with the brainstemthe part that houses the breathing centercan spark CSA. Here are the usual suspects:
- Stroke: Especially strokes that hit the brainstem, where the respiratory rhythm is set.
- Parkinsons disease and related disorders such as multiple system atrophythese affect the nerves that convey the breathing signal.
- Brain tumors or traumatic brain injuries: They can physically compress or disrupt the respiratory nuclei.
- Spinal cord lesions that affect the pathway between the brain and diaphragm.
According to a review in the , patients with these conditions often develop CSA as a secondary complication, making early detection crucial.
Cardiac / Vascular Causes
Heart problems are the second most common driver of CSA, particularly in people with chronic heart failure. The mechanism is called CheyneStokes respiration: an unstable feedback loop between carbon dioxide levels and heart output.
- Congestive heart failure: Reduced cardiac output leads to delayed circulation of CO, prompting overcompensation and then a pause.
- Atrial fibrillation: Irregular heart rhythms can disturb the timing of blood flow to the brain, affecting the breathing center.
- Hypertension: Longterm high blood pressure can remodel the brains vasculature and alter respiratory control.
Studies from the show that treating the heart condition often reduces the frequency of central apneas dramatically.
Metabolic & Systemic Causes
Beyond brain and heart, a few system issues can tip the balance.
- Endstage renal disease: Dialysis can cause rapid shifts in CO, provoking central apneas.
- Thyroid disorders (both hyper and hypothyroidism) can alter the sensitivity of the respiratory drive.
- High altitude: The thinner air reduces oxygen, which can trigger central pauses in susceptible individuals.
Secondary Contributing Triggers
Even if you dont have a major heart or brain condition, certain habits and medicines can nudge you toward CSA.
MedicationInduced CSA
Opioids are the biggest culprits. They blunt the brains response to CO, essentially telling the breathing center to chill out. Even lowdose prescriptions for chronic pain can be enough.
Benzodiazepines and other sedativehypnotics have a similar effect, especially when combined with alcohol.
TreatmentRelated CSA
Ever heard of complex sleep apnea? Its when someone treated for OSA with CPAP suddenly develops central apneas. The positive pressure can overcorrect airway obstruction, leading the brain to think it doesnt need to breathe.
Lifestyle & Environmental Factors
While not primary causes, smoking, binge drinking, and large fluctuations in body weight can worsen underlying instability in the breathing system. If youre living at a high altitude (think mountainous towns), you might notice more pauses on clear nights.
Idiopathic Central Sleep Apnea
Sometimes, doctors run all the tests, rule out heart disease, brain lesions, medications, altitude and still find CSA. Thats called idiopathic central sleep apnea. It accounts for roughly 510% of CSA cases.
What Makes It Idiopathic?
In these cases, the exact trigger is unknown. Researchers suspect a genetic predisposition that makes the respiratory control system overly sensitive or unstable. Ongoing studies are probing the role of certain neurotransmitters and even the gut microbiome.
RealWorld Example
Meet Samantha, a 48yearold graphic designer with no heart issues, no stroke history, and who doesnt take opioids. She started noticing morning headaches and daytime sleepiness. A sleep study showed a high central apnea index, but every medical workup was clean. Her physician labeled it idiopathic CSA, and after a trial of adaptive servoventilation (ASV), her symptoms improved dramatically.
Danger of These Causes
So, why does any of this matter? Simply put: untreated CSA can be risky.
Immediate Health Risks
- Sudden drops in blood oxygen (desaturation) during sleep.
- Frequent arousals that prevent deep, restorative sleep.
- Daytime fatigue, poor concentration, irritability.
LongTerm Complications
Research published in the indicates that individuals with CSA linked to heart failure have about a 20% higher allcause mortality rate compared to those without CSA. The chronic lowoxygen environment can fuel hypertension, worsen arrhythmias, and increase stroke risk.
Diagnosing the Underlying Cause
Getting to the root of CSA is a bit like detective workyou need the right clues.
Sleep Study (Polysomnography)
The gold standard is an overnight polysomnogram. It records brain waves, oxygen levels, airflow, and chest movements. Technicians look for the central apnea index (CAI)the number of central events per hour. A CAI 5 typically confirms CSA.
Cardiac WorkUp
If the sleep study shows many central events, the next step is usually a cardiac evaluation: echocardiogram, BNP blood test, and possibly a stress test to gauge heart function.
Neurological Imaging
When neurological causes are suspected, an MRI or CT scan of the brain can reveal strokes, tumors, or demyelinating lesions.
Laboratory Panels
Thyroid function tests, renal panels, and a drug screen help rule out metabolic or medicationrelated contributors.
Checklist for Your Doctor Visit
- Bring a sleep diary (bedtimes, awakenings, symptoms).
- List every medication and supplement you take.
- Note any recent surgeries, head injuries, or heart events.
- Ask about a possible overnight pulseoximeter test if a lab sleep study isnt feasible.
Treatment Options by Cause
Once the trigger is identified, treatment becomes much more targeted.
Treat the Heart
Optimizing heartfailure therapyACE inhibitors, betablockers, diureticsoften reduces CSA frequency. For patients with CheyneStokes breathing, an adaptive servoventilation (ASV) machine can smooth out the breathing pattern by delivering pressure support only when the pause is detected.
Treat Neurological Triggers
If Parkinsons disease is the root, adjusting dopaminergic meds can improve respiratory control. Poststroke rehabilitation often includes breathing exercises as part of neurorecovery protocols.
Medication Adjustments
Talk to your prescriber about tapering opioids or switching to nonopioid pain relievers. For sedatives, a gradual reduction or a switch to a less respiratorysuppressive agent can make a world of difference.
General & Natural Approaches
While lifestyle tweaks arent a cure, they can help:
- Sleep on your side and elevate the head of the bed a few inches.
- Avoid alcohol and heavy meals within two hours of bedtime.
- If you live at high altitude, consider a shortterm stay at lower elevation.
- Practice paced breathing or yoga nidrajust remember these are supportive, not primary treatments.
According to the , these natural steps can improve sleep quality but should always accompany a medical plan.
When No Clear Cause Is Found
For idiopathic CSA or cases where the underlying problem cant be fully corrected, device therapy remains the backbone:
- CPAP may work for some, especially if theres a mixed OSA/CSA picture.
- Bilevel PAP (BiPAP) provides different pressures for inhalation and exhalation and can be easier to tolerate.
- Supplemental nocturnal oxygen is sometimes prescribed for highaltitude or hypoventilation cases.
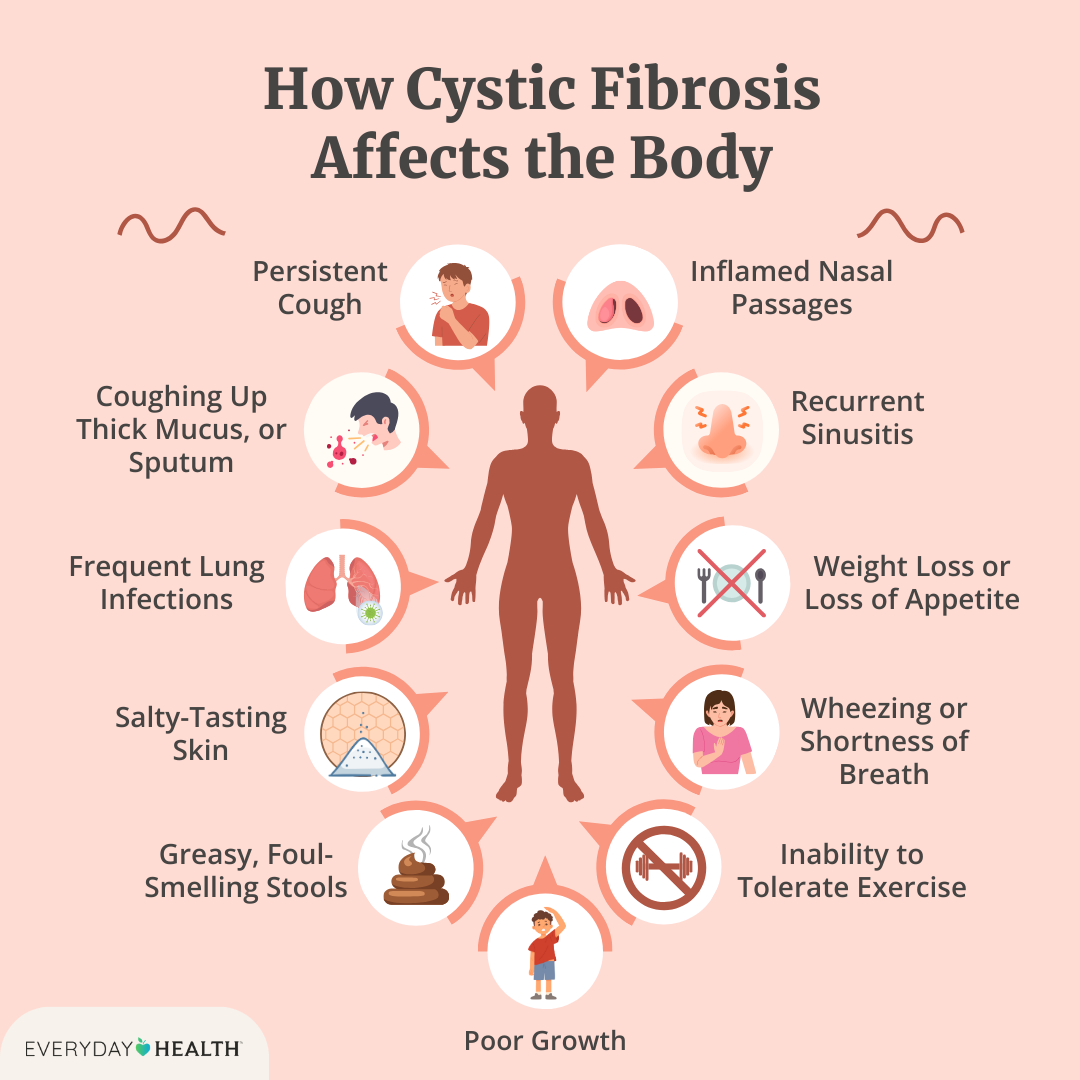
People with chronic lung conditions sometimes need tailored airway strategies; for resources on airway management techniques, see this guide on cystic fibrosis airway clearance which covers airway clearance methods and chest physiotherapy approaches that can be adapted to specific respiratory needs.
Quick FAQ Highlights
Can central sleep apnea be cured?
Most people see big improvements when the underlying cause is treated. Cure depends on the causeheartrelated CSA often gets better with cardiac therapy; idiopathic cases usually need lifelong device support.
Is central sleep apnea dangerous?
Yes. Untreated CSA can lower oxygen levels, increase blood pressure, and raise the risk of heart disease and stroke.
What are the neurological causes of central sleep apnea?
Strokes, Parkinsons disease, brainstem lesions, tumors, and traumatic brain injuries can all disrupt the brains breathing signal.
How does central sleep apnea differ from obstructive sleep apnea?
CSA is a signaling problemno effort to breathe. OSA is a blockageyour body tries, but the airway is closed.
Are there natural treatments for central sleep apnea?
Lifestyle changes like sleeping upright, avoiding alcohol, and altitude adjustments can help, but theyre adjuncts to medical carenot replacements.
Bottom-Line Takeaways
- Central sleep apnea is usually a sign that the heart, brain, or certain meds are out of sync.
- It can be seriouslow oxygen and heart strain are real risks.
- Accurate diagnosis (sleep study + medical workup) is essential.
- Treating the root causewhether heart failure, a stroke, or medicationoffers the best chance for relief.
- Device therapies like ASV, CPAP, or BiPAP are effective when the cause cant be fully fixed.
If any of this resonates with youor if youve noticed strange pauses in your sleepdont wait. Talk to a sleep specialist or your primary doctor. A quick evaluation could save you from future health trouble and get you back to feeling rested, energized, and ready for whatever the day brings. Got questions or a story to share? Drop a comment below; Id love to hear how youre tackling sleep health!
FAQs
What are the most common causes of central sleep apnea?
The leading causes include heart failure (especially Cheyne‑Stokes respiration), brainstem strokes or lesions, Parkinson’s disease, opioid or sedative use, and high‑altitude exposure.
How does heart failure lead to central sleep apnea?
Reduced cardiac output delays CO₂ removal, creating an unstable feedback loop that triggers over‑compensation followed by a pause in breathing, known as Cheyne‑Stokes respiration.
Can medications like opioids cause central sleep apnea?
Yes. Opioids blunt the brain’s response to rising CO₂ levels, suppressing the respiratory drive and often producing central apneas even at low doses.
Is there a cure for central sleep apnea?
When the underlying condition (e.g., heart failure, stroke, medication) can be treated, the apnea often improves dramatically. In idiopathic cases, lifelong device therapy such as ASV or CPAP may be needed.
What treatment options are available for central sleep apnea?
Treatment may involve optimizing heart‑failure meds, adjusting or tapering offending drugs, using adaptive servo‑ventilation (ASV), BiPAP, CPAP, supplemental oxygen, or lifestyle changes like sleeping upright and avoiding alcohol.