Feeling that nagging ache just below your rib cage? You might be wondering if its something simple like indigestion or something a bit more specific, like a problem in the prepyloric region. In the next few minutes Ill walk you through exactly what this part of your stomach does, why it can get irritated, and what you can do about itno medical jargon, just plain, friendly advice.
What is Prepyloric
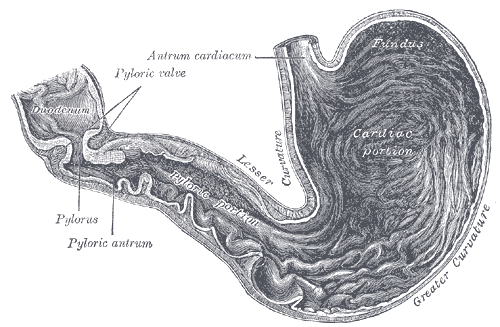
Anatomy in Plain Words
The prepyloric region sits at the very end of the stomach, right before the narrow passage called the pyloric canal leads food into the duodenum. Think of it as the gateway that regulates how quickly the stomach empties. Because its so close to the duodenum, its exposed to both strong stomach acid and the early digestive enzymes that start working on your meal.
How It Differs From Other Stomach Parts
Most people hear about stomach ulcers in general, but ulcers that form in the prepyloric area behave a bit differently. Theyre more likely to resist standard H2blocker medications and can sometimes progress to more serious conditions if not caught early. Thats why a clear understanding of this specific region matters.
Quick Comparison
| Region | Typical Issues | Treatment Preference |
|---|---|---|
| Fundus | Acid hypersecretion | PPIs, lifestyle changes |
| Antrum | H. pylori infection | Triple therapy |
| Prepyloric | Ulcers, gastritis, perforation | PPIs, endoscopic therapy, sometimes surgery |
Prepyloric Ulcer
What It Is
A prepyloric ulcer is an open sore that develops in that gateway area. Its part of the broader category of peptic ulcer disease, but its location gives it a unique set of symptoms and risks.
Typical Symptoms
Most people describe a burning or gnawing pain that shows up a few hours after eating, especially on an empty stomach. Other common clues include:
- Nausea or a feeling of fullness after just a bite
- Vomitingsometimes with a hint of blood
- Unexplained weight loss
- Heartburn that doesnt improve with antacids
Why It Happens
Three big culprits usually show up on the list:
- H.pylori infection a bacteria that weakens the stomach lining.
- NSAID use everyday painkillers like ibuprofen can erode the protective mucous layer.
- Lifestyle factors smoking, heavy alcohol use, and chronic stress.
According to a study published in , the prepyloric area is particularly prone to ulcer formation when H.pylori is present because the bacteria tend to congregate near the pyloric sphincter.
When to Call the Doctor
If you notice any of the following, treat them as red flags:
- Sudden, severe abdominal pain that spreads to the back (possible prepyloric perforation)
- Vomiting blood or material that looks like coffee grounds
- Persistent vomiting or inability to keep food down
These symptoms demand immediate medical attentiondont wait.
Diagnosis & Testing
Endoscopy: The Gold Standard
A prepyloric stomach endoscopy lets a gastroenterologist look directly at the ulcer. The procedure involves a thin tube with a camera that slips down your throat, letting the doctor spot the sore, take biopsies, and even treat it on the spot.
What Doctors Look For
During the session theyll note the ulcers size, depth, and whether theres any surrounding inflammation (often called prepyloric gastritis). Theyll also assess the pyloric sphincters functionto see if its closing too tightly or too loosely.
Biopsy: When Tissue Tells the Story
A prepyloric region biopsy is usually performed if the ulcer looks suspicious, if theres persistent pain despite treatment, or if theres a family history of gastric cancer. The tiny tissue sample is examined under a microscope for H.pylori, dysplasia, or even early cancer cells.
Additional Tests
Beyond endoscopy, doctors may order:
- A urea breath test or stool antigen test for H.pylori.
- Blood work to check for anemia or inflammation.
- A CT scan if they suspect a perforation or deep tissue involvement.
Treatment Options
FirstLine Medical Management
Most prepyloric ulcers respond well to proton pump inhibitors (PPIs). These meds block acid production more effectively than the older H2blockers, which tend to be less reliable in the prepyloric zone. A typical course lasts 812 weeks.
H.pylori Eradication
If testing shows the bacteria, a tripletherapy regimenusually a PPI plus two antibiotics (clarithromycin and amoxicillin or metronidazole)is prescribed. Follow the schedule exactly; missing doses can let the bug bounce back.
Endoscopic Therapy
When medication alone isnt enough, an endoscopist can apply heat (thermal coagulation), inject medication directly into the ulcer, or clip the tissue to seal the wound. These techniques have a success rate of 7080% for stopping bleeding and promoting healing.
When Endoscopy Fails
If the ulcer persists after several rounds of medication and endoscopic effort, surgery might be consideredespecially if theres a risk of prepyloric perforation or if you develop chronic bleeding.
Surgical Interventions
Most surgeons now prefer minimally invasive (laparoscopic) approaches. Options include a wedge resection of the ulcerated area or a partial gastrectomy if the ulcer is large or suspected to be cancerous. Recovery typically takes 46 weeks, with a gradual return to normal diet.
Complications & Prognosis
Perforation: A Serious Emergency
A hole in the stomach wallprepyloric perforationlets stomach contents leak into the abdominal cavity, causing intense pain, fever, and a rapid drop in blood pressure. Its a surgical emergency with a mortality rate of about 10% if not treated quickly.
Bleeding and Anemia
Chronic ulcer bleeding can lead to irondeficiency anemia. If you notice persistent fatigue, pale skin, or shortness of breath, ask your doctor to check your blood count.
Risk of Cancer
While most prepyloric ulcers are benign, longstanding inflammation can increase the chance of gastric carcinoma. A study in found that ulcers in the prepyloric zone have a slightly higher malignant transformation rate than those elsewhere in the stomach.
LongTerm Outlook
With proper treatmentusually a combination of PPIs, H.pylori eradication, and lifestyle tweaksmost patients recover fully within a few months. Regular followup endoscopies are advised for highrisk individuals, especially if youve had a biopsy showing dysplasia.
Lifestyle & Prevention
Diet Tips that Help
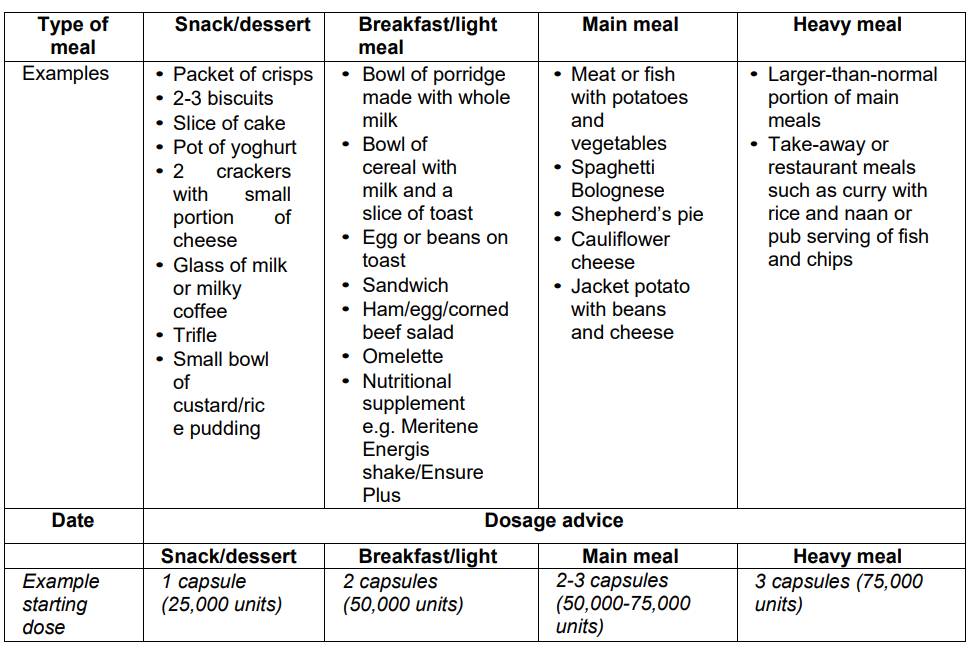
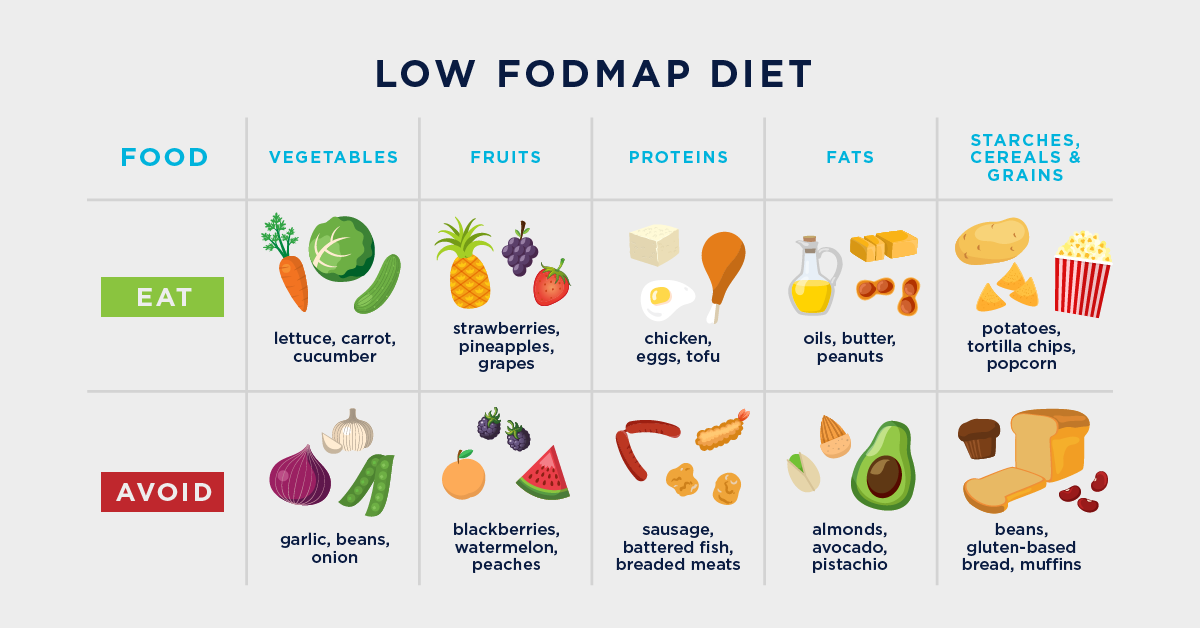
Skimp on the spicy, acidic, and fried foods for a while. Opt for bland, easytodigest meals like oatmeal, steamed veggies, and lean proteins. Small, frequent meals can also keep the stomach from overproducing acid.
Medication Management
If you need NSAIDs for chronic pain, talk to your doctor about using the lowest effective dose or switching to acetaminophen. A pill organizer or a reminder app can keep you on track with your PPIs.
Quit Smoking & Limit Alcohol
Both smoking and heavy drinking weaken the stomachs protective lining. Cutting back can dramatically lower the chance of an ulcer returning.
FollowUp Biopsies
For anyone whos had a prepyloric region biopsy showing atypical cells, doctors usually schedule repeat biopsies at 6month intervals for the first year, then yearly after that. This proactive approach catches any early changes before they become serious.
Some patients with chronic digestive conditions also benefit from broader digestive support; for example, reading about gentle gluten detox approaches can help those who suspect food triggers while they pursue definitive testing.
Key Takeaways
The prepyloric region may be a tiny slice of your digestive tract, but it plays a massive role in keeping food moving smoothly from stomach to intestine. When its irritated, you might feel a lingering gnaw, occasional nausea, or worse, signs of bleeding or perforation. The good news? Most issues are treatable with a mix of medication, endoscopic care, and, when needed, surgery. By staying alert to symptoms, getting timely diagnosticslike a prepyloric stomach endoscopyand adopting healthier habits, you can keep this gateway running without a hitch.
Got questions about your own symptoms or the best treatment plan? Drop a comment below or reach out to a gastroenterology specialistyou deserve clear answers and a stomach that feels comfortable again.