Quick Treatment Summary
Think of treating adrenocortical carcinoma (ACC) as a three-part recipe:
- Surgery the main dish that can be curative when the tumor is removed completely.
- Adjuvant therapy radiation or chemotherapy added after surgery to mop up any hidden cells.
- Systemic options drugs that travel through the bloodstream, used when surgery isnt enough or the cancer has spread.
Heres a quick-hit table that shows what typical doctors recommend at each stage.
| Stage | Typical First Move | Common Follow-Up |
|---|---|---|
| III | Radical adrenalectomy (open or laparoscopic) | Observation or adjuvant mitotane if high-risk features |
| III | Surgery + adjuvant radiation | EDP-mitotane chemotherapy |
| IV | Systemic therapy (EDP-mitotane, clinical trial) | Palliative radiation or surgery for symptom control |
Staging Drives Choices
The stage tells the whole story. ACC is staged using the TNM system (tumor size, lymph node involvement, metastasis). The later the stage, the more likely youll need a combination of treatments.
What are the hallmark symptoms of stage-4 ACC?
When the cancer spreads, patients often notice new pain near the back, unexplained weight loss, and in some cases, hormone-related signs like high blood pressure or skin darkening. These are the classic stage4 adrenal cancer symptoms that signal its time to talk about systemic therapy.
How do treatment guidelines differ by stage?
Both the NCCN and other specialty guidelines publish detailed adrenocortical carcinoma treatment guidelines. In short, early-stage disease leans heavily on surgery, while later stages call for more aggressive chemotherapy and, when possible, participation in clinical trials. For patients curious about long-term outcomes after major surgery, resources discussing prostate removal life expectancy can sometimes help frame recovery expectations after organ-removing procedures, though the specifics differ by cancer type.
Surgery as Cornerstone
If theres any silver lining, its that removing the tumor can actually cure a good number of patientsprovided the surgeon gets clean margins (no cancer cells left at the edge of the cut). Thats why the phrase radical adrenalectomy pops up so often in the literature.
What does a radical adrenalectomy involve?
During an open adrenalectomy, the surgeon makes a sizable incision to see the gland clearly and remove it en bloc with surrounding tissue. Laparoscopic surgery uses small ports and a camera, offering faster recovery but only when the tumor isnt too large or invasive.
When is surgery not feasible?
If the tumor has invaded major blood vessels or spread widely, an operation might do more harm than good. In those cases, doctors pivot to chemotherapy, targeted drugs, or palliative radiation to keep symptoms in check.
Real-world example
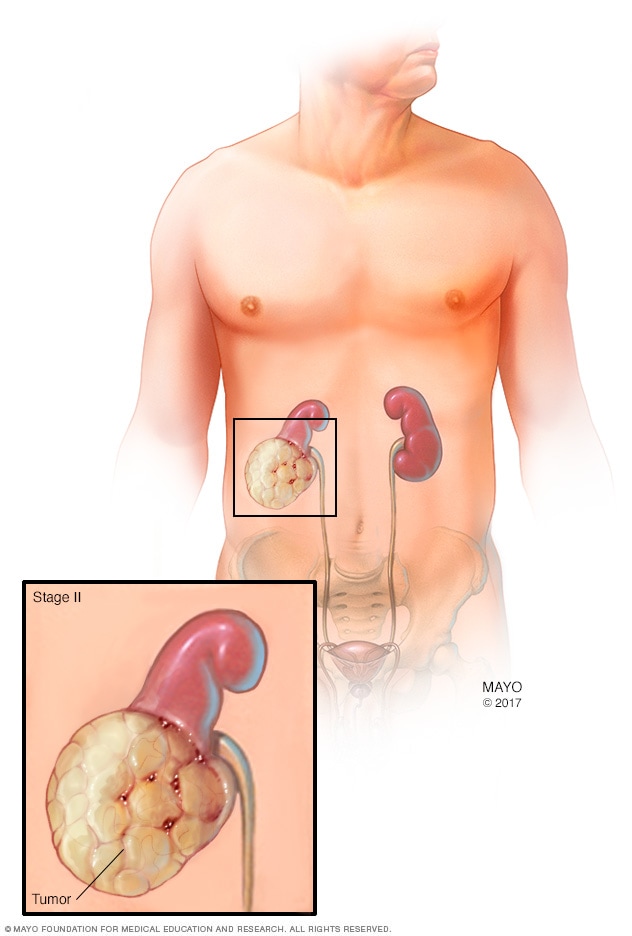
Consider Sarah, a 45-year-old teacher diagnosed at stage II. Her surgical team performed a laparoscopic adrenalectomy, and she was home in three days. Pathology showed clean margins, and she now enjoys a cancer-free life five years latera testament to how surgery can be both curative and life-changing.
Radiation Therapy Role
Radiation isnt a cure for ACC, but it can shrink tumors that cant be removed safely, and it helps prevent recurrence after surgery.
Is radiation curative for ACC?
No, its mostly an adjuvant (after-surgery) or palliative tool. High-dose IMRT (intensity-modulated radiation therapy) or SBRT (stereotactic body radiation) can control local disease and relieve pain.
Typical side-effects & mitigation
Patients may feel fatigue, skin redness, or nausea. Proper planning and supportive medslike antiemetics and skin creamskeep those side-effects manageable.
Chemotherapy Options Overview
The backbone of systemic therapy for ACC is the EDP regimen (etoposide, doxorubicin, cisplatin) combined with mitotane, a drug that specifically targets adrenal cortex cells.
What is the EDP-mitotane regimen?
Patients receive these three chemo drugs every three weeks, while mitotane is taken daily. Blood levels of mitotane are monitored closely because the therapeutic window is narrow; too low, and it wont work; too high, and you risk severe toxicity.
How effective is mitotane alone?
Mitotane can slow tumor growth on its own, especially for hormone-secreting tumors, but it rarely clears the disease completely. Think of it as a maintenance medication, similar to thyroid hormone replacement after the gland's removed.
Emerging systemic options
Researchers are testing immune checkpoint inhibitors (pembrolizumab, nivolumab) and tyrosine-kinase inhibitors (cabozantinib) in trials. Early data show modest response rates, but for patients who have exhausted standard options, these new treatments for adrenal cancer offer a glimmer of hope.
Emerging New Treatments
Clinical trials are the lifeline for rare cancers like ACC. In 2024, the First International Randomized Trial in Locally Advanced and Metastatic ACC (FIRMACT) reported a modest increase in overall survival when patients received a combination of pembrolizumab with standard EDP-mitotane.
Are there FDA-approved new drugs?
As of early 2025, no brand-new drug has received full FDA approval specifically for ACC, but several are in Phase II/III trials. If youre looking for an edge, ask your oncologist about enrolment in a trialespecially if you fall into the stage4 adrenocortical carcinoma prognosis category.
How do genetics influence therapy?
Mutations in TP53 or CTNNB1 can make tumors more aggressive. Some centers are beginning to tailor therapy based on these genetic clues, a step toward precision medicine that may soon affect which adrenocortical carcinoma treatment drug you receive.
Balancing Benefits & Risks
Every treatment carries tradeoffs. Below is a simple matrix that helps weigh the pros and cons of each option.
| Modality | Key Benefits | Major Risks |
|---|---|---|
| Surgery | Potential cure, rapid symptom relief | Bleeding, organ injury, postop adrenal insufficiency |
| Radiation | Local control, pain reduction | Fatigue, skin changes, rare organ damage |
| EDP-Mitotane Chemo | Improves survival in stage III/IV | Neutropenia, nausea, mitotane-induced adrenal crisis |
| Immunotherapy (Trials) | Potential for durable responses | Immune-related colitis, hepatitis, thyroiditis |
When you sit down with your oncology team, bring a notebook, ask about each risk, and discuss how youd manage side-effects together. Shared decision-making is the cornerstone of trustworthy, patient-centered care.
Survival Rates & Prognosis
ACC is rare, and that makes statistics feel a bit like a puzzle. Overall 5-year survival hovers around 30%, but it varies dramatically by stage:
- Stage I: >70% 5-year survival
- Stage II: ~50%
- Stage III: 2030%
- Stage IV: <15%
These numbers come from the latest NCI data (2024). The key takeaway? Early detection and complete surgical removal dramatically shift the odds in your favor.
What does the prognosis look like for stage-4?
When ACC has metastasized, the focus often shifts to extending life and preserving quality. Median overall survival is roughly 1218 months with aggressive chemo, but patients who enroll in clinical trials can sometimes beat that benchmark.
How does treatment improve survival?
Studies consistently show that patients who receive adjuvant mitotane after a clean resection enjoy a 1015% increase in 5-year survival compared with surgery alone. In lay terms, thats the difference between maybe Ill see my grandkids and Ill definitely be there for them.
Trusted Resources & Help
Finding reliable information is half the battle. Here are a few go-to sources that keep their facts straight and are easy to navigate:
- uptodate treatment guidelines and trial listings.
- American Association of Cancer Researchers (AACR) patient forumsreal stories from people walking the same road.
- Endocrine Societys clinical practice guidelinesespecially useful for hormone-related symptoms.
How to verify a reliable source?
Look for three things: affiliation with a recognized institution (e.g., NCI, NCCN), recent publication date (within the last 23 years), and citations of peer-reviewed studies. If a site meets all three, you can trust the numbers they present.
Questions to ask your oncologist
- What stage is my tumor, and how does that affect my treatment options?
- Am I a candidate for adjuvant mitotane, and what blood levels should we aim for?
- Are there any clinical trials currently recruiting that match my profile?
- What supportive care services (nutrition, endocrine replacement, counseling) are available?
Having these questions ready shows youre engaged and helps the doctor give you the most relevant information.
Conclusion
In a nutshell, treating adrenocortical carcinoma is a step-by-step journey. Surgery is the foundation, radiation and chemotherapy add layers of protection, and newer drugsplus clinical trialsoffer hope when standard options fall short. The key is a personalized plan that balances potential benefits with the reality of side-effects, guided by clear, trustworthy information.
Weve covered the basics, the numbers, and the newest developments, and I hope you feel a bit more empowered to navigate this daunting landscape. If you or someone you love is facing ACC, reach out to a specialized center, ask about trials, and lean on support groupsno one should walk this path alone.
FAQs
What is the main treatment for adrenocortical carcinoma?
Surgery is the primary treatment for adrenocortical carcinoma, especially when the tumor can be removed completely.
When is chemotherapy used for adrenocortical carcinoma?
Chemotherapy is typically used for advanced or metastatic adrenocortical carcinoma, often in combination with mitotane.
Can radiation therapy cure adrenocortical carcinoma?
Radiation therapy is not curative but can help control local disease and relieve symptoms after surgery or in advanced cases.
Are there new treatments for adrenocortical carcinoma?
New treatments like immunotherapy and targeted drugs are being tested in clinical trials for adrenocortical carcinoma.
What is the survival rate for stage 4 adrenocortical carcinoma?
The 5-year survival rate for stage 4 adrenocortical carcinoma is less than 15%, but treatment can improve quality of life.