What Is Cardiotoxicity?
Definition and basic science
Cardiotoxicity refers to the harmful effects that some chemotherapy drugs, radiation, or targeted therapies can have on the heart muscle and its electrical system. This damage can lead to reduced heart pumping ability (lower ejection fraction), arrhythmias, or even heart failure. Think of the heart as a car engineif you pour the wrong fuel in, it may run for a while but eventually sputters, and the longer you wait, the harder it is to fix.
How common is it?
Recent data from the CARDIOTOX Registry (2024) show that up to 9% of patients receiving highdose anthracyclines develop clinically significant cardiotoxicity, while milder changes in heart function can be seen in as many as 30% of patients undergoing combined chemoradiation. Those numbers may sound high, but the good news is that early detection and treatment dramatically improve outcomes.
Types of Cardiotoxicity
| Type | When It Appears | Typical Symptoms | Common Culprit Drugs |
|---|---|---|---|
| Acute | During or immediately after treatment | Chest pain, arrhythmia, sudden drop in blood pressure | Doxorubicin, trastuzumab |
| Chronic | Months to years later | Shortness of breath, fatigue, swelling of ankles | Anthracyclines, chest radiation |
Who Is At Risk?
Highrisk treatments
Not every chemo drug hurts the heart, but a handful are notorious:
- Doxorubicin (and other anthracyclines) the classic cardiotoxicity drug.
- Trastuzumab (Herceptin) a targeted therapy for HER2positive breast cancer.
- Chest radiation especially when the heart lies in the radiation field.
Patientspecific factors
Even if youre on a lowrisk regimen, other things can tip the scales:
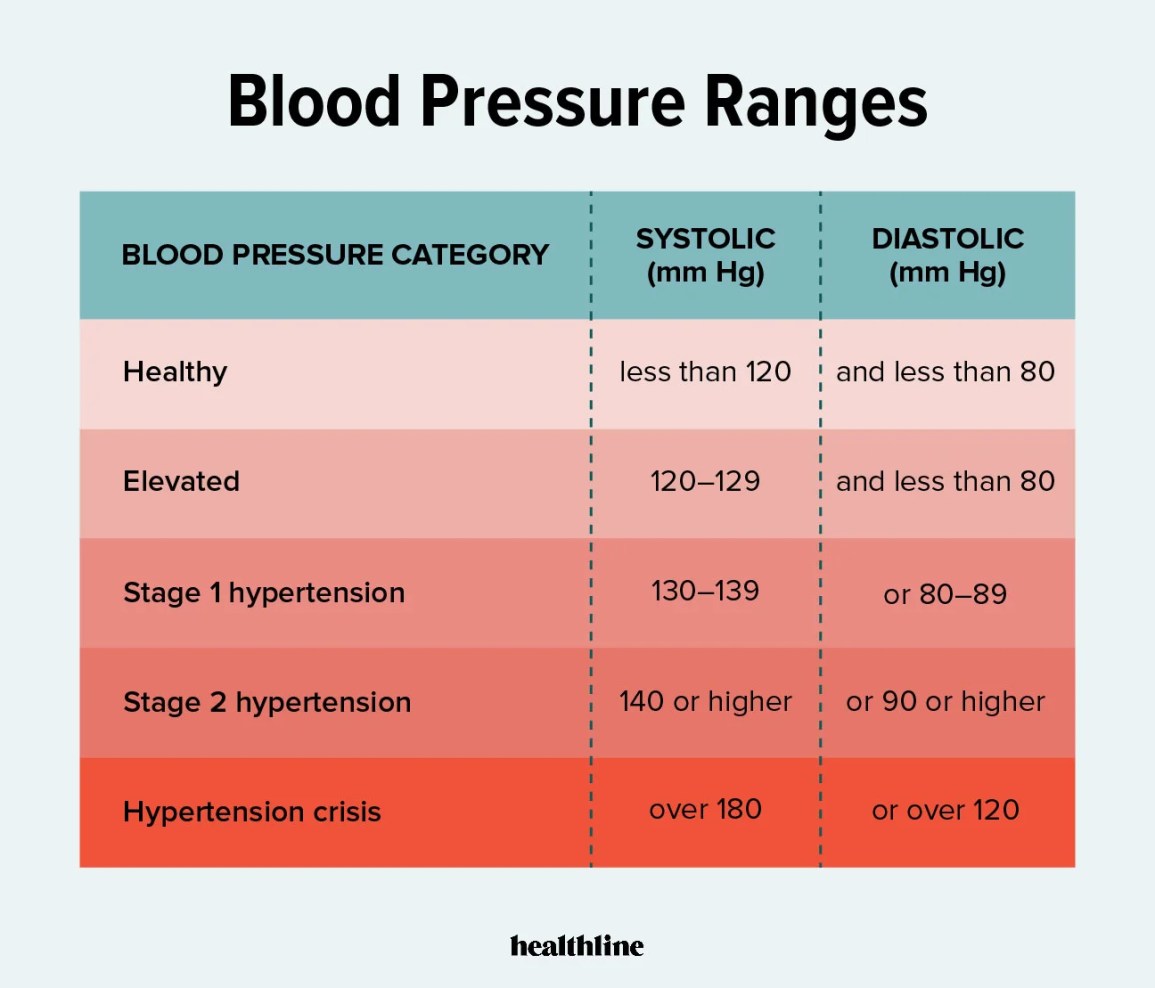
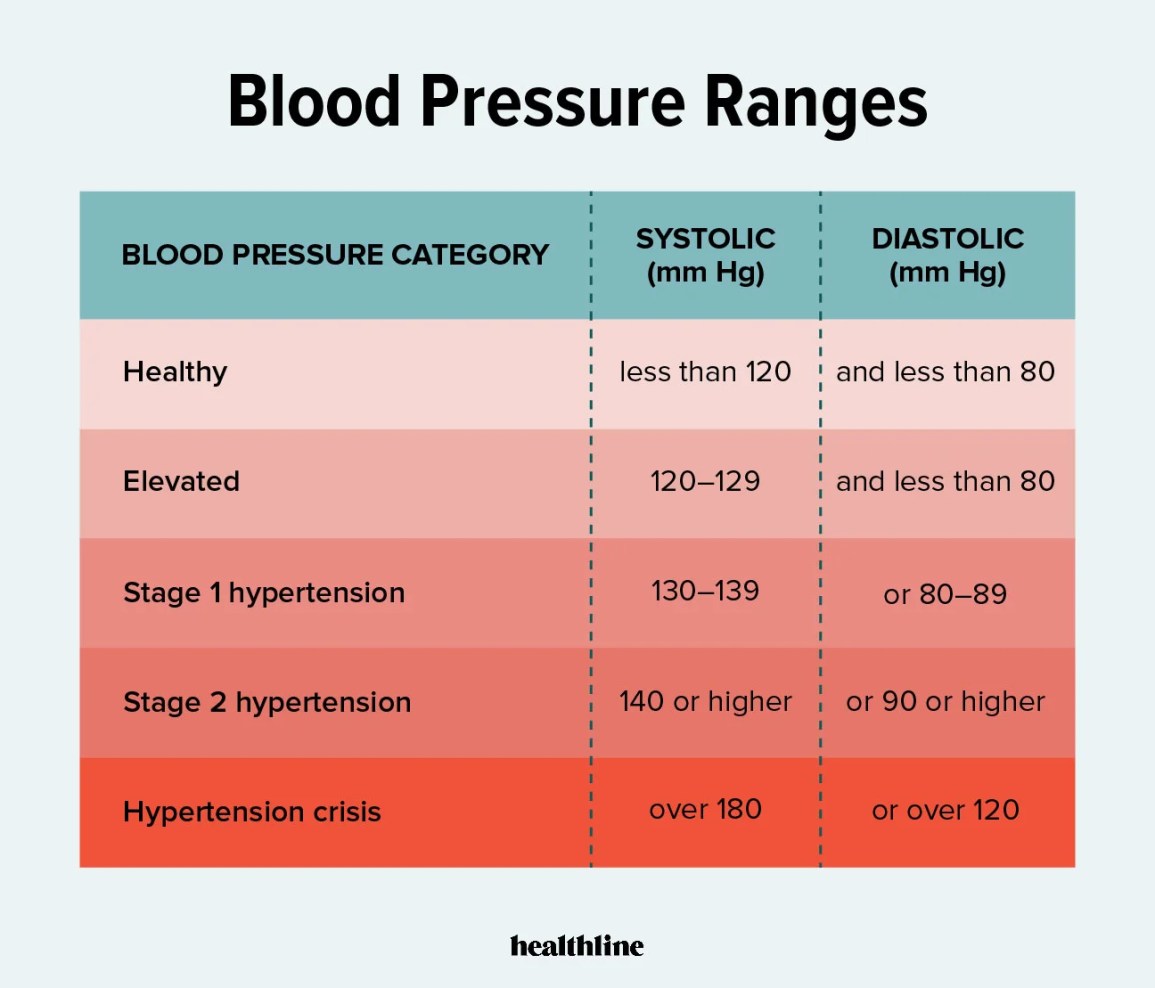
- Preexisting heart disease, high blood pressure, or diabetes.
- Older age or very young age (children treated with anthracyclines often develop issues later in life).
- Cumulative dose exceed a certain amount of doxorubicin (about 450mg/m) and the risk climbs sharply.
Realworld case
Take Maria, a 45yearold who finished six cycles of doxorubicin for lymphoma. Three years later she started feeling unusually winded climbing stairs. An echo showed a modest drop in leftventricular function. Early intervention with an ACEinhibitor slowed the decline, and today shes back to hiking with her kids.
Symptoms of Cardiotoxicity
Early warning signs
The body rarely shouts heart damage! but it does whisper. Keep an ear out for:
- Unexplained shortness of breath, even at rest.
- Persistent fatigue that doesnt improve with rest.
- Swelling in the ankles, feet, or abdomen.
- Irregular heartbeats or palpitations.
- Chest discomfort that feels different from typical chemo nausea.
When symptoms mimic other conditions
Its easy to mistake cardiotoxicity symptoms for anemia, asthma, or even anxiety. Thats why a quick check with your doctor is essential, especially if symptoms develop during or after treatment.
Symptom checklist (quick scan)
- Shortness of breath?
- Fatigue beyond chemo tired?
- Swollen ankles?
- Fluttering heart?
- Chest pressure?
How Cardiotoxicity Is Diagnosed
Imaging tests
An echocardiogram is the first line it measures the leftventricular ejection fraction (LVEF) and can spot subtle changes. Some centers use strain imaging, a more sensitive technique that catches early muscle dysfunction before LVEF falls.
Biomarkers
Blood tests for troponin and Btype natriuretic peptide (BNP) can flag heart injury even when imaging looks normal. Rising troponin during chemo is a red flag that warrants closer monitoring.
ICD10 coding for proper documentation
When you or your clinician documents cardiotoxicity, the appropriate code isI51.9 Cardiac disease, unspecified. Using the correct code ensures your insurance covers followup care and helps researchers track realworld outcomes.
Sample note (expertlevel illustration)
Patient presents with dyspnea on exertion 3 months postdoxorubicin. Echo shows LVEF 48% (baseline 60%). Troponin elevated. Diagnosis: I51.9 cardiotoxicity. Initiated lisinopril 5mg daily.
Managing Cardiotoxicity Treatment
Pharmacologic options
When heart function drops, drugs that protect the heart step in:
- ACEinhibitors (e.g., lisinopril) lower blood pressure and reduce remodeling.
- Betablockers (e.g., carvedilol) calm the hearts rhythm and improve pumping efficiency.
- Dexrazoxane a chelator specifically approved to mitigate anthracyclinerelated damage.
Lifestyle tweaks that help
Hearthealthy habits are powerful allies. Aim for a Mediterraneanstyle diet rich in leafy greens, omega3 fish, and whole grains. Moderate aerobic activity (like brisk walking) a few times a week boosts circulation without overtaxing a vulnerable heart. And quit smoking if you havent already every puff adds extra stress.
Adjusting cancer therapy
Sometimes the oncologist may lower the chemo dose, switch to a lesscardiotoxic agent, or pause treatment while the heart recovers. That decision is always a balance of beating cancer and protecting the heart. According to a study published in , patients whose treatment was modified based on early cardiac monitoring had a 30% lower rate of severe heart failure.
Is cardiotoxicity reversible?
Earlystage damage often improves with medication and lifestyle changes. In many anthracycline cases, LVEF can bounce back by 510% within a year of starting ACEinhibitors. However, chronic fibrosis (scar tissue) may be permanent, underscoring the value of catching it early.
Success stories (experience)
James, a 60yearold with lung cancer, experienced mild chest tightness after four cycles of carboplatin-paclitaxel. A prompt echo revealed a dip to 52% LVEF. With carvedilol and a revised chemo schedule, his LVEF rebounded to 58% and he completed treatment without further heart issues.
How to Prevent Cardiotoxicity
Baseline heart check before chemo
Guidelines from the American Society of Clinical Oncology (ASCO) recommend a full cardiac workupincluding echo and biomarkersbefore starting any known cardiotoxic regimen. This baseline tells the care team what normal looks like for you, making future changes easier to spot.
Ongoing monitoring schedule
A typical surveillance plan might look like this:
- Echo + troponin before each major chemo cycle (or every 23 cycles).
- Repeat echo 3 months after finishing treatment, then annually for at least 5 years.
- Prompt repeat if any cardiotoxicity symptoms appear.
Emerging protective agents
Researchers are testing antioxidants, mitochondrial protectors, and even geneediting techniques to shield heart cells. While most are still in clinical trials, they signal a hopeful future where cancer cures wont cost the heart.
DrugSpecific Prevention Strategies
| Drug | Prevention | Key Monitoring |
|---|---|---|
| Doxorubicin (anthracycline) | Dexrazoxane, limit cumulative dose, ACEinhibitor prophylaxis | Echo + troponin before each cycle |
| Trastuzumab (HER2 blocker) | Baseline echo, betablocker if risk factors | Echo every 3 months during therapy |
| Chest radiation | Heartsparing techniques, lifestyle hearthealth | Echo 612 months postradiation, then annually |
Resources & Help
Trusted medical centers
Institutions like the Cleveland Clinics CardioOncology program and the MD Anderson Cancer Center have dedicated teams that specialize in preventing and treating cardiotoxicity. Their multidisciplinary approach ensures your oncologist and cardiologist speak the same language.
Patient advocacy groups
The American Heart Associations CardioOncology section offers webinars, printable monitoring guides, and a community forum where survivors share tips. Connecting with others can turn a scary diagnosis into a shared journey.
Talking to your care team
Dont wait for a symptom to pop up. Bring up the following questions at your next appointment:
- What baseline cardiac tests do I need before starting chemo?
- How often should we repeat heart imaging while Im on treatment?
- Are there preventive medications you recommend for my specific regimen?
Conclusion
Cardiotoxicity may feel like an unwelcome surprise in the cancer journey, but with the right knowledge it becomes a manageable part of your treatment plan. Remember the three pillars: recognize the warning signs, get regular heart monitoring, and act early with proven treatments or lifestyle tweaks. By staying proactive, you give your heart the best chance to stay strong while you focus on beating cancer. If you have questions about your own risk or want to (chat) about strategies, reach out to your cardiology or oncology teamyou deserve clear, caring guidance every step of the way.
For patients noticing persistent swelling in the ankles or legs as part of cardiotoxicity, consider learning more about causes and management of fluid buildup for example, approaches to leg swelling cause can overlap with heartfailure edema strategies and help guide early discussions with your care team.
FAQs
What is cardiotoxicity?
Cardiotoxicity is heart damage caused by certain cancer treatments, such as chemotherapy or radiation, which can impair heart function and lead to symptoms like shortness of breath or fatigue.
Which cancer treatments cause cardiotoxicity?
Drugs like doxorubicin, trastuzumab, and chest radiation are common causes of cardiotoxicity, but other therapies including targeted agents and immunotherapies may also pose risks.
How is cardiotoxicity diagnosed?
Cardiotoxicity is diagnosed using imaging tests like echocardiograms to measure heart function and blood tests for biomarkers such as troponin and BNP.
Can cardiotoxicity be prevented?
Yes, prevention includes baseline heart checks, regular monitoring during treatment, and sometimes using protective medications like dexrazoxane or ACE inhibitors.
Is cardiotoxicity reversible?
Early-stage cardiotoxicity is often reversible with prompt treatment, but chronic damage such as heart muscle scarring may be permanent.