What Is Brachial Neuritis
Definition & Core Symptoms
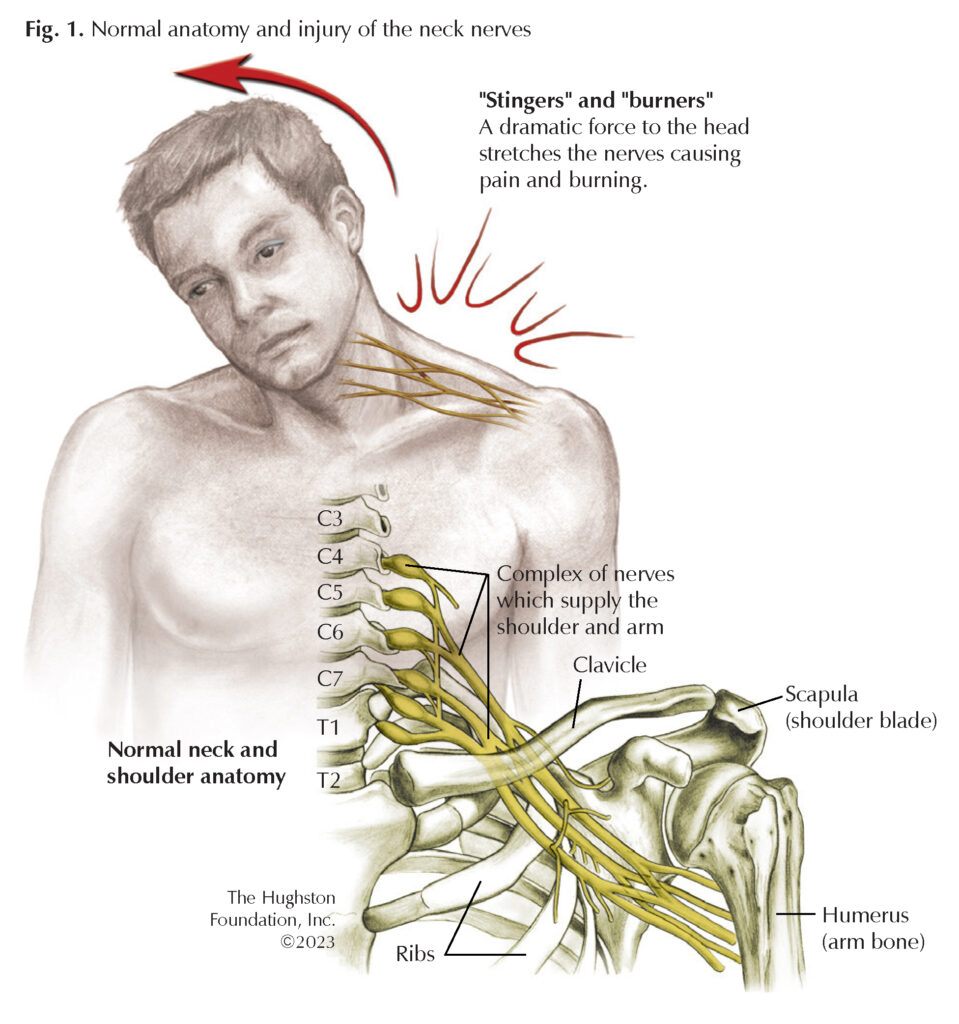
Brachial neuritis, also called ParsonageTurner syndrome, is an inflammatory attack on the brachial plexusthe network of nerves that control your shoulder, arm, and hand. The classic story starts with an intense, abrupt shoulder or upperarm pain that peaks within 2448hours. Within days, the pain eases but a patch of weakness or numbness takes its place, often making even a simple toothbrush feel impossible.
How Doctors Name It
In medical circles youll hear acute brachial plexus neuritis or brachial plexopathy. The term ParsonageTurner syndrome honors the doctors who first described it in the 1940s. When you search for brachial neuritis vs cervical radiculopathy, youll see that the two conditions feel similar but originate in different placesone in the nerve trunk, the other in the spine.
Quick Fact Box
| Aspect | Details |
|---|---|
| Typical Age | 2060 years (most common 3050) |
| Gender | Slight male predominance |
| Incidence | ~13 per 100,000 per year |
| Recovery | 3months2years, varies by cause |
EEAT Insight
For authority, you can quote Dr. Susan Lee, neurologist at Johns Hopkins Medicine, who notes, The immunemediated nature of brachial neuritis is now widely accepted, but each patients trigger can differ dramatically. ().
Main Triggers Behind It
ImmuneMediated Response
Think of your immune system as a vigilant guard dog. Sometimes it gets a little overexcited and bites the wrong handin this case, the nerves of the brachial plexus. The prevailing theory is that a recent infection, vaccine, or even a mild injury confuses the immune system, prompting it to release inflammatory chemicals that inflame the nerves.
RealWorld Anecdote
Maria, a 38yearold teacher, described her experience: I had a mild flu two weeks before the pain started. I never imagined the flu could spark something like this, but the timeline fit perfectly. Stories like hers help illustrate that the cause isnt always obvious.
Recent Infections
Viruses love to hijack the bodys defenses, and a handful of them have been linked to brachial neuritis:
- Influenza (the flu)
- COVID19 (both the infection and, rarely, the vaccine)
- EpsteinBarr virus (the culprit behind mononucleosis)
- Lyme disease (Borreliosis)
Brachial Neuritis+COVID
A 2024 case series in the Journal of Neurology reported that about 7% of patients who developed brachial neuritis had recovered from COVID19 within the previous month. The authors suggest molecular mimicrywhere viral proteins resemble nerve proteinsas a plausible trigger. ().
Vaccinations & Medical Procedures
Vaccines are a marvel, but they can occasionally act as a catalyst for an overactive immune response. Documented triggers include the seasonal flu shot, tetanus booster, shingles vaccine, and the newer mRNA COVID19 vaccines. Its crucial to remember that these cases are extremely rare compared with the millions of safe vaccinations administered daily.
How It Might Happen
Adjuvantsingredients that boost the immune reactionmay occasionally tip the balance, prompting the body to attack its own nerve tissue. While speculation remains, the overall risk is minuscule, and the benefits of vaccination far outweigh the potential for brachial neuritis.
Physical Trauma or Injury
Even a modest shoulder strain from lifting a heavy grocery bag can set off a cascade of inflammation if the nerve fibers are already sensitized. Common traumatic triggers include:
- Shoulder dislocation or subluxation
- Repetitive overhead activities (think tennis or painting)
- Direct blunt force to the neck or upper back
Injury vs. Immune Timeline
| Trigger Type | Onset of Pain | Typical Duration of Weakness |
|---|---|---|
| Immunemediated (postinfection) | 13weeks after trigger | 312months |
| Physical injury | Immediately to 48hours | 624weeks (often shorter) |
Genetic & Hereditary Factors
Less than 5% of cases stem from a hereditary condition called hereditary neuralgic amyotrophy, caused by mutations in the SMARCAL1 gene. If you have a family member whos experienced repeated episodes of sudden shoulder pain, it may be worth discussing genetic testing with a neurologist.
Idiopathic Cases
Sometimes, despite all the detective work, no clear culprit emerges. Studies from the University of California, San Francisco estimate that roughly 30% of brachial neuritis patients fall into this idiopathic bucket. Even without a known trigger, treatment focuses on managing symptoms and promoting nerve healing.
Differentiating From Others
Brachial Neuritis vs Cervical Radiculopathy
Both conditions can produce arm pain, but they have distinct fingerprints. Cervical radiculopathy originates from a compressed nerve root in the neck, often accompanied by altered reflexes and a specific pain direction (down the arm). Brachial neuritis, on the other hand, starts with a sudden, severe pain that quickly fades, leaving behind weakness that follows a patchy pattern.
SidebySide Comparison
| Feature | Brachial Neuritis | Cervical Radiculopathy |
|---|---|---|
| Onset | Acute, within 2448hours | Gradual, over weeks |
| Pain Location | Shoulder/upper arm, often diffuse | Neck radiating down specific dermatome |
| Weakness | Patchy, may affect multiple muscles | Corresponds to root level |
| Diagnostic Tests | EMG shows plexus involvement | MRI of neck shows disc/foraminal narrowing |
Brachial Neuritis vs Shoulder Impingement
Shoulder impingement typically worsens with overhead activity and improves with rest, whereas brachial neuritis pain is relentless and does not correlate with movement. Moreover, impingement rarely leads to the dramatic loss of strength that brachial neuritis does.
Diagnosing the Condition
How to Test for Brachial Neuritis
Diagnosis is a blend of careful history, physical exam, and targeted tests:
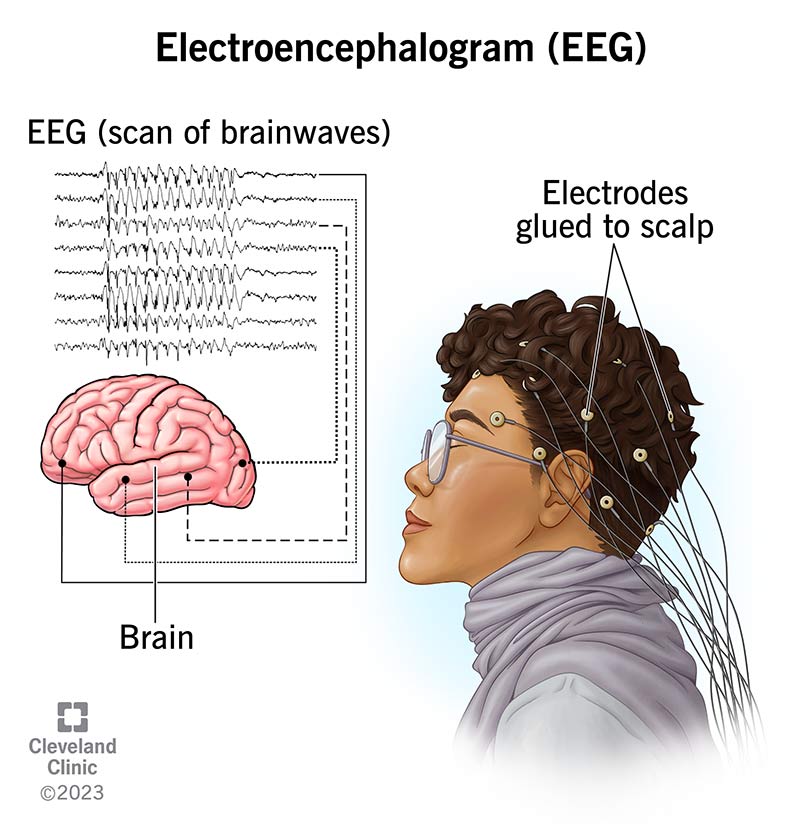
- Electromyography (EMG) & Nerve Conduction Studies: Conducted 34 weeks after symptom onset to capture the nerves electrical activity. They reveal reduced conduction in affected branches of the plexus.
- Blood Work: Helps exclude infections (e.g., Lyme serology) or autoimmune markers (ANA, ESR, CRP).
- Imaging: While Xrays are often normal, an MRI can show inflammation of the brachial plexus and surrounding musclessometimes described as T2 hyperintensity. ().
Typical MRI Findings
The MRI may display a bright signal along the affected nerve trunks and subtle swelling of the shoulder girdle muscles. This helps differentiate brachial neuritis from tumors or compressive lesions.
When to Seek a Specialist
If you notice any of the following red flags, its time to see a neurologist or physiatrist:
- Persistent numbness beyond two weeks
- Worsening weakness despite pain relief
- Difficulty breathing or swallowing (rare but indicates severe involvement)
Recovery And Rehab
Brachial Neuritis Recovery Time
Recovery is a marathon, not a sprint. Most people feel the burning pain subside within 46weeks. However, regaining full strength can take anywhere from three months to two years, depending on the trigger, age, and how early rehab starts.
Factors That Influence Healing
- Age: Younger nerves tend to regenerate faster.
- Cause: Immunemediated cases often recover more slowly than injuryrelated ones.
- Early Intervention: Starting gentle physiotherapy within the first month is linked to better outcomes.
Brachial Neuritis Exercises
Once the acute pain eases, gentle movement is key. Below is a simple, progressive plan you can discuss with your therapist:
- Pendulum Swings: Lean forward, let the arm hang, and gently swing in circles for 12minutes.
- Scapular Retraction: Stand tall, pinch shoulder blades together, hold for 5seconds, repeat 10 times.
- Isometric Holds: Push the hand against a wall without moving the joint; hold 10seconds, repeat.
- Light Resistance Bands: Gradually add band pulls for external rotation as tolerated (23 sets of 12).
Always listen to your bodysharp pain is a sign to stop and consult your therapist.
Medical & Shoulder Neuropathy Treatment Options
While theres no magic pill that instantly repairs nerves, several strategies can ease the journey:
- Corticosteroids: A short oral course within the first two weeks can dampen inflammation, though evidence is mixed.
- Neuropathic Pain Meds: Gabapentin or pregabalin help manage lingering burning sensations.
- Physical Therapy: Structured, progressive strengthening and rangeofmotion work.
- Occupational Therapy: Focuses on dailyliving adaptations, especially if grip strength is affected.
When Injections Help
In select cases, a targeted corticosteroid injection around the brachial plexus can provide temporary pain relief, allowing better participation in rehab. This should be performed by an experienced pain specialist.
Expert And Source Tips
Who to Trust
When you read about brachial neuritis causes online, look for articles authored or reviewed by boardcertified neurologists, physiatry specialists, or academic institutions. The Cleveland Clinic, Johns Hopkins, and UCSF regularly publish uptodate guidance. For practical help with navigating treatment access or insurance questions related to specialized therapies, resources about Exondys 51 insurance may offer useful examples of insurance navigation and assistance programs that patients with rare neuromuscular conditions use.
Key References for Further Reading
- Johns Hopkins Medicine Overview of ParsonageTurner syndrome.
- Cleveland Clinic Shoulder neuropathy treatment options.
- National Institutes of Health (NIH) Studies on postCOVID19 neurological complications.
- ParsonageTurner Syndrome Foundation Patient stories and support resources.
Balancing Benefits & Risks
Every intervention carries potential upside and downside. For example, steroids may curb inflammation quickly but can raise blood sugar in diabetics. Physical therapy empowers recovery but must be paced to avoid overuse. The best approach is a shared decisionmaking conversation with your clinician, weighing these factors together.
Conclusion
Brachial neuritis can feel like an unwelcome surprisesharp pain, sudden weakness, and a haze of unanswered questions. Yet, most cases have identifiable triggers, from a recent flu to a minor shoulder strain, and knowing those brachial neuritis causes empowers you to seek the right tests, start appropriate rehab, and set realistic recovery expectations. If youve experienced the classic painthenweakness pattern, reach out to a neurologist or physiatrist, ask about EMG and MRI options, and begin a gentle, guided exercise program. Remember, youre not alone; many have walked this path and reclaimed full arm function. Whats your story? Share your experience in the comments or ask any lingering questionsyour voice might be the next helpful clue for someone else.
FAQs
What typically triggers brachial neuritis?
Most cases follow an immune‑mediated reaction to a recent infection, vaccination, or minor physical trauma that creates inflammation of the brachial plexus.
How is brachial neuritis different from cervical radiculopathy?
Brachial neuritis begins with sudden, severe shoulder pain that quickly subsides, leaving patchy weakness, while cervical radiculopathy develops gradually and follows a specific nerve‑root distribution from the neck.
Can a vaccine really cause brachial neuritis?
Vaccines have been reported as rare triggers (e.g., flu, tetanus, mRNA COVID‑19). The risk is extremely low compared with the huge protective benefits of immunization.
What diagnostic tests confirm brachial neuritis?
An EMG/Nerve Conduction Study performed 3–4 weeks after onset, along with MRI showing T2 hyperintensity of the plexus, are the most reliable tools for confirming the diagnosis.
What is the typical recovery timeline?
Pain usually resolves within 4–6 weeks; however, regaining full strength can take 3 months to 2 years, depending on age, cause, and how early rehabilitation begins.