Okay, lets cut to the chase: the first line of defense for reactive arthritis is usually a short course of NSAIDs to tame the pain and swelling, and antibiotics only join the party if theres an active infection still hanging around. Below youll find a stepbystep guide that walks you through medicines, lifestyle tweaks, how long the flareup might last, and the myths that keep popping up.
Grab a cup of tea, settle in, and lets untangle everything you need to know about managing reactive arthritis so you can get back to the things you lovewithout feeling like youre reading a textbook.
Understanding the Condition
What is reactive arthritis?
Reactive arthritis is a form of joint inflammation that shows up after an infection elsewhere in the bodythink a stomach bug, a urinary tract infection, or a chlamydia infection. Your immune system, trying to clear the invader, accidentally turns its fire on the joints, usually the knees, ankles, or feet. Its a classic postinfectious reaction: the bug is gone, but the joint pain hangs around.
Is it an autoimmune disease?
Thats a great question because the terminology can get confusing. Reactive arthritis is immunemediated, not a classic autoimmune disease like rheumatoid arthritis. In autoimmune disorders, the body attacks itself continuously, whereas in reactive arthritis the immune response is triggered by a recent infection. , the condition usually subsides once the immune system calms down.
How long does reactive arthritis last?
Most people see the acute phase melt away in about 36months. Around 1020% may develop chronic joint pain that lasts a year or longer, and a very small slice can experience recurring flares. If youre wondering whether its permanent, the good news is that the majority recover fully, especially with early treatment and lifestyle support.
Quick comparison: Reactive vs. Rheumatoid Arthritis
| Feature | Reactive Arthritis | Rheumatoid Arthritis |
|---|---|---|
| Trigger | Recent infection (GI, GU, respiratory) | Autoimmune, no infection trigger |
| Joint pattern | Asymmetric, often lower extremities | Symmetric, often hands & wrists |
| Typical labs | Elevated ESR/CRP, HLAB27 positive in many | RF/antiCCP antibodies often present |
| Course | Usually selflimited, can become chronic | Chronic, progressive if untreated |
Core Medical Treatments
Firstline: NSAIDs
Nonsteroidal antiinflammatory drugs (NSAIDs) like ibuprofen, naproxen, and indomethacin are the goto for most flareups. They shrink swelling, ease stiffness, and let you move without feeling like youve been hit by a truck. Start with the lowest effective dose and take them with food to protect your stomach. If you have high blood pressure or kidney issues, chat with your doctor before committing.
When antibiotics are needed
The phrase reactive arthritis treatment antibiotics pops up a lot, but antibiotics only make sense if the original infection is still alive. For example, a lingering chlamydia infection calls for a course of azithromycin or doxycycline. If your bout was a foodborne bug like Salmonella, a short course of ciprofloxacin might be prescribed. In most cases, once the infection clears, antibiotics stop being useful and can actually fuel resistance.
Corticosteroids
If NSAIDs arent enough, a doctor may sprinkle in a short burst of oral steroids (like prednisone) or inject a corticosteroid directly into the painful joint. This can dramatically cut inflammation within days. Remember, steroids are powerfuluse them sparingly and follow a tapering schedule to avoid rebound flareups.
DMARDs and Biologics
For the minority whose arthritis sticks around past the acute phase, diseasemodifying antirheumatic drugs (DMARDs) such as sulfasalazine or methotrexate step in. They work slowerweeks to monthsbut they target the underlying immune activity. If youre still symptomatic after several months, a biologic that blocks tumor necrosis factor (TNF) may be considered. recommends a stepwise approach, starting with NSAIDs and moving up only if needed.
Treatment decision flowchart (in words)
1Acute joint pain start NSAIDs.
2Check for active infection add antibiotics if needed.
3No response in 12weeks consider short steroids.
4Symptoms linger >3months evaluate DMARDs or biologics.
5Throughout add PT, diet, and lifestyle support.
Supporting Lifestyle Therapies
Physical therapy & joint protection
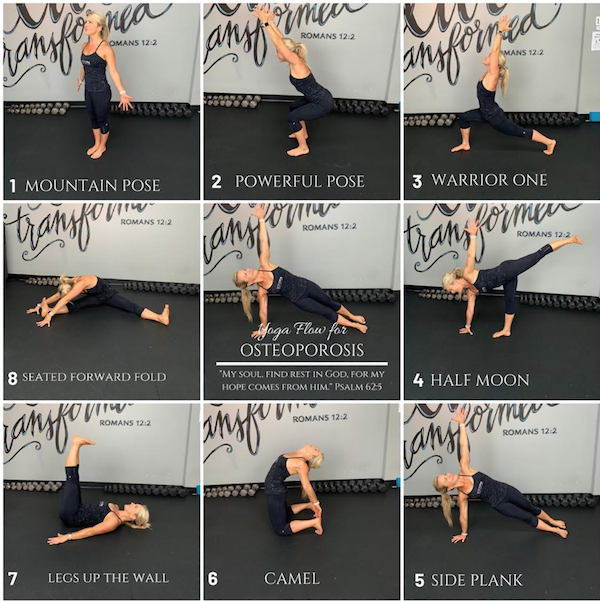
Movement may feel like an enemy right now, but gentle rangeofmotion exercises keep joints from stiffening. A physical therapist can teach you lowimpact movesthink swimming, cycling, or yogatailored to your pain level. Supporting your joints with braces or compression sleeves during flareups can also help reduce stress.
Reactive arthritis diet
Theres no magic diet that cures the condition, but an antiinflammatory eating plan can calm the fire. Load up on omega3rich foods (salmon, walnuts, flaxseed), vibrant fruits and veggies, and spices like turmeric or ginger. Cut back on refined sugars, processed snacks, and excessive alcohol, which can aggravate inflammation. Staying hydrated and maintaining a healthy weight also lessen the load on your knees and ankles.
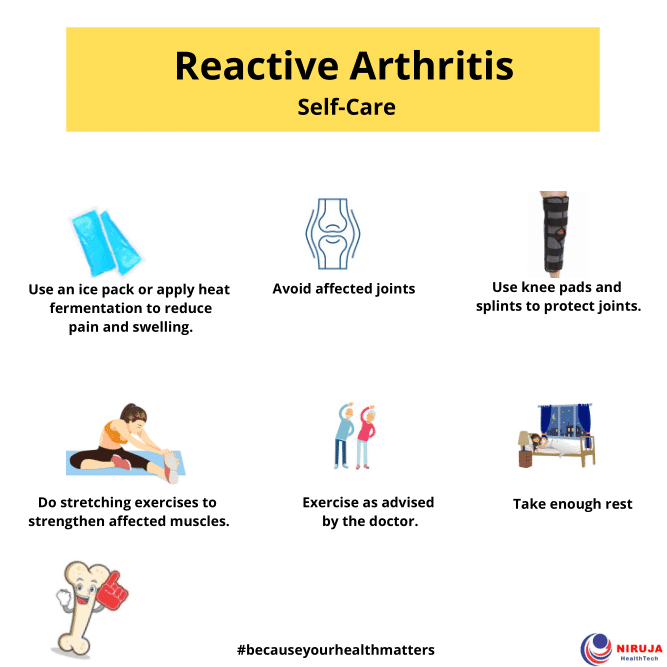
Managing pain & fatigue at home
Heat packs, ice packs, and gentle massage can bring fast relief. Overthecounter acetaminophen may help if NSAIDs irritate your stomach. For fatigue, short naps, balanced meals, and light activity (a brisk walk) often beat staying in bed all day. Listen to your bodypush when you feel good, rest when you dont.
Is the condition permanent?
Most folks bounce back. A shows that about 8090% of patients see their symptoms fade within a year. A small group may have lingering joint discomfort that needs ongoing management, but its rarely permanent in the sense of a lifelong, unchanging disability.
Checklist: What to tell your doctor
- Recent infections (GI, GU, respiratory)
- Exact start date of joint pain
- Current medications, including overthecounter drugs
- Any pregnancy plans or breastfeeding status
- Allergies or prior reactions to NSAIDs or steroids
Diagnosis Process Overview
Clinical criteria
Doctors look for the classic triad: arthritis (often in the knees or ankles), conjunctivitis (red eye), and urethritis (painful urination). Not everyone shows all three, but at least two clues plus a recent infection usually seal the deal. If you suspect a related chronic condition such as ankylosing spondylitis remission is a treatment goal or differential, mention persistent back pain or stiffness to your clinician so they can consider the appropriate diagnostic criteria and follow-up.
Lab work
Typical labs include a CBC, ESR or CRP (to gauge inflammation), and a test for HLAB27, a genetic marker that shows up in about 70% of cases. If a bacterial trigger is suspected, urine PCR for chlamydia or stool cultures for Salmonella may be ordered.
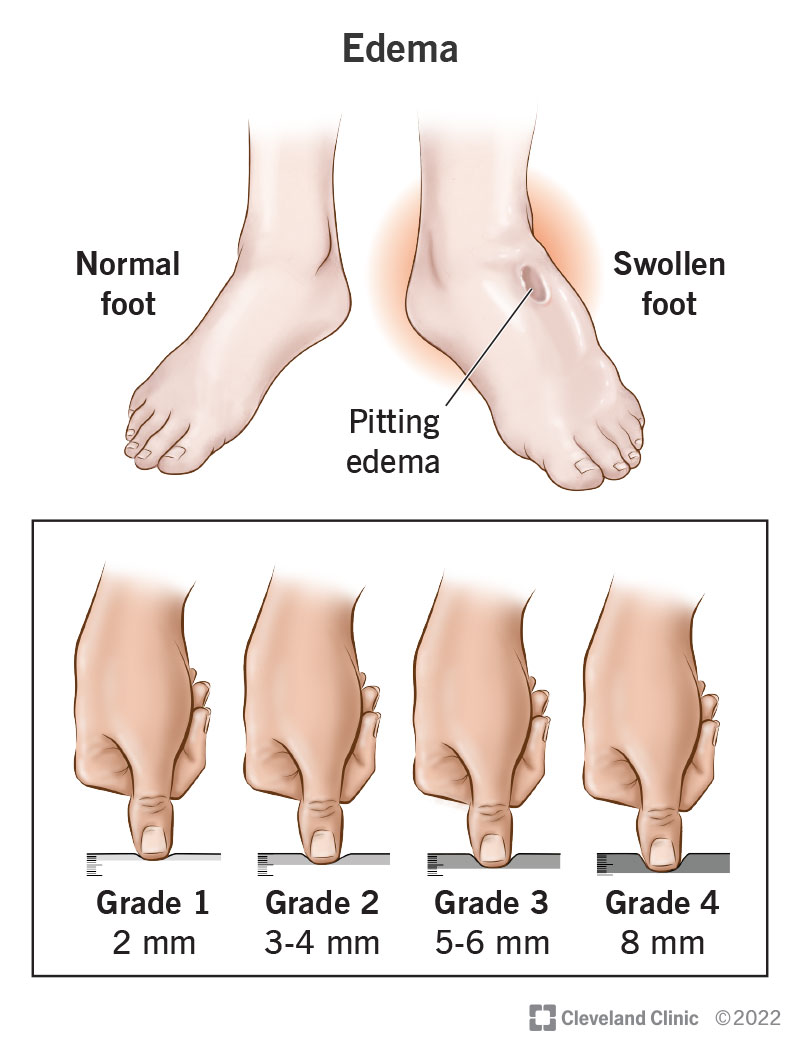
Imaging
Xrays often look normal early on, but an ultrasound can spot joint effusion (fluid) and early cartilage changes. MRI is reserved for stubborn cases where you need a detailed view of soft tissues.
Diagnostic algorithm (in words)
Suspected symptoms clinical exam blood tests (ESR/CRP, HLAB27) infection testing imaging if needed diagnosis treatment plan.
Balancing Benefits & Risks
Potential sideeffects of NSAIDs & steroids
NSAIDs can irritate the stomach lining, raise blood pressure, or affect kidney function, especially if you take them longterm. Steroids might cause mood swings, higher blood sugar, or weight gain. Thats why you should always use the lowest effective dose for the shortest time and keep your doctor in the loop.
Antibiotic resistance concerns
Using antibiotics when theres no active infection can fuel resistant bugssomething we all want to avoid. Thats why clinicians reserve reactive arthritis treatment antibiotics for proven, ongoing infections only.
When to seek urgent care
If you notice sudden, severe joint swelling, a fever over101F, vision changes, or a painful red eye that wont go away, head to urgent care. Those could be signs of a complicated infection or an extraarticular manifestation that needs rapid treatment.
Riskmitigation tips
- Take NSAIDs with food or a protonpump inhibitor if you have stomach issues.
- Ask your doctor for regular blood tests when on DMARDs.
- Complete any prescribed antibiotic courseno shortcuts.
- Report new symptoms promptly; early tweaks prevent bigger problems.
Resources Next Steps
Reliable online portals
Trusted sites like , the , and the NHS all offer uptodate guides and patient stories.
Support groups & forums
Connecting with others whove walked the same road can be a lifeline. The Arthritis Foundations community forums, r/Arthritis on Reddit, and local patientsupport groups give you a space to share tips, vent frustrations, and celebrate small victories.
When to schedule a specialist appointment
If symptoms linger beyond three weeks despite NSAIDs, or if you experience eye redness, skin rashes, or persistent fever, its time to see a rheumatologist. Early specialist care can finetune your treatment plan and prevent chronic joint damage.
Downloadable quickreference sheet
Weve put together a handy PDF you can printthink of it as your reactive arthritis cheat sheet. It includes the treatment algorithm, a symptomlog template, and a list of foods to try (or avoid). and keep it on your fridge for quick reference.
Managing reactive arthritis is a mix of smart medication choices, lifestyle tweaks, and staying in sync with your healthcare team. The journey isnt always smooth, but with the right tools and a dash of patience, many people find their pain eases and they get back to doing the things they love.
Got a story about how a certain diet or exercise helped you through a flare? Share it in the commentsyour experience could be the exact tip someone else needs. And if you have any lingering questions, feel free to ask; were all in this together.
FAQs
What are the first‑line medicines for reactive arthritis?
NSAIDs such as ibuprofen, naproxen, or indomethacin are usually prescribed first to reduce pain and inflammation.
When are antibiotics necessary in reactive arthritis treatment?
Antibiotics are only needed if the original infection (e.g., chlamydia, Salmonella) is still active; they are not useful once the trigger has been cleared.
How long does a reactive arthritis flare usually last?
The acute phase typically resolves within 3‑6 months, though 10‑20 % of people may experience symptoms that persist longer.
Can lifestyle changes help manage reactive arthritis symptoms?
Yes. An anti‑inflammatory diet, regular low‑impact exercise, weight control, and joint‑protective strategies can all lessen pain and improve function.
When should I see a rheumatologist for reactive arthritis?
Seek a specialist if pain continues beyond three weeks despite NSAIDs, or if you develop eye redness, skin rashes, fever, or chronic joint swelling.